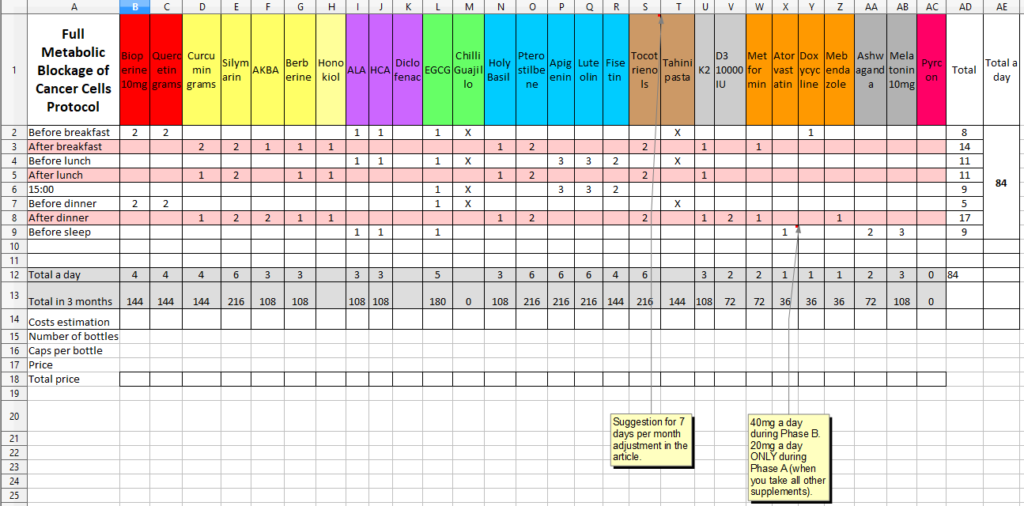
Vertical version of the table above
Full Metabolic Blockage Protocol
– Main Outcome
– Dosage and time of use
– Who is suitable for the protocol?
– Tailoring the protocol ingredients
– RED zone – bio boosters
– YELLOW zone – curcumin and synergistic ingredients
– VIOLET zone – Laurent Schwartz METABLOC protocol
– GREEN zone – D. James Morré EGCG protocol
– BLUE zone – The Magnificent Five
– BROWN zone – tocotrienols + sesamine
– GREY zone – vitamin K2 + D3
– ORANGE zone – COC protocol
– BLACK zone – Bedtime
– PINK zone – Pyrcon
What we may consider to add to the protocol – candidates? (For specific cancers; Maybe; No; Avoid at all costs)
What blood values to monitor during the protocol?
Possible targets of individual substances in the protocol
– ORANGE zone – Fatty Acids Metabolism
– RED zone – Glucose Metabolism
– BLUE zone – Glutamine Metabolism
– Targeting Cholesterol
– Inhibiting the growth of new blood vessels
– Evasion of anti-growth signaling
– When tumor cells metastasize
– Chronic inflammation
– Journey to immortality – make them mortals again
– Other targets
Other useful information
Off-topic. Why we don’t have a cure yet?
Q&A – your questions from Facebook answered
If you like this article, you can buy me a coffee. Thank you!
PayPal.Me/fullmetabolic
Before we begin… let’s be honest
This protocol has never been tried before – it is purely experimental. There are experiences with COC protocol alone, but the combination suggested here has never being tried by anyone. Close to 100 supplement pills per day is extreme daily dosage. It is impossible to predict any side effects (including alergies, interactions with other drugs you take etc.), as there are too many variables, making it too complex.
I have been researching cancer topic since 2014 and written over 120 articles which are published on my Czech website ww.alternativnicesta.cz. All content has always been published for free (I didn’t use any ads, any embedded referral links etc.). My main goal has been to deliver (attempting to deliver) objective information about alternative treatments and to warn about the biggest quacks and scammers who are just trying to make money on the illness (which is common). I would be completely honest: I hate those people. Nothing is lower than making money on selling false claims when you know they are people out there seeking for hope, trying to save themselves or their beloved. They are becoming easy targets for confident lies.
This protocol contains the very best from what I have come across during the whole journey. But even though I did put thousands of hours into it, it is still only my 6 years old child. It is still a baby.
I’m not a doctor. I studied sociology and psychology at the university. I have tried to employ my ability to process information, sort them, linked them together and transfer into understandable form. This journey has been extremely difficult for me, as I had very little information about the human body. I have tried to do my best and you can judge on your own if I succeded or failed.
But it is your life, your health. Is trying my best good enough? Be sceptical. My interpretations presented may be incorrect or misleading. This protocol is a theoretical approach, and the premises can be wrong. I still know only little, after 6 years of study. Also I could have been cherry picking to make foundations hold. I could have misunderstood some info etc.
So be sceptical, verify everything, take the text as inspiration, as a collection of information which I have arduously collected for you.
Always consider standard medical treatment as the first option. It is currently the best choice available for the kill phase.
This protocol is complementary and if you assess the background theory as valid, you could opt in and follow after the kill phase is completed. Or you can use it as a pre-treatment (before you start your main treatment).
It is so easy to succumb to “internet anecdotes” as they are all written so confidently and present themselves as “sure cure” when there is none.
Be wary about random internet texts about cancers, which are showing too much confidence. There is no confidence in writing about cancers, only unreflected Dunning-Kruger effect.
They are hundreds of people around cancer, to whom we can apply biblical: Beware of false prophets, which come to you in sheep’s clothing, but inwardly they are ravening wolves.
Full Metabolic Blockage Protocol
First layer is COC which are 4 repurposed drugs currently used for other diagnoses. These are metformin, atorvastatin, mebendazole and doxycycline. They are one of the pillars of this protocol
- CareOncologyClinic homepage
- CancerTreatmentResearch article
- METRICS clinical study NCT02201381
- Jane McLelland Off Label Drugs for Cancer Public Group (Facebook)
- Jane McLelland How to Starve Cancer book
Second layer is METABLOC, a protocol invented by French oncologist Laurent Schwartz which consists of Alpha Lipoic Acid and Hydroxycitric Acid (extracted from Garcinia Cambogia).
Recent suggestion presented in Peres, 2019 recommends to add also metformin (already part of the COC) and diclofenac (over the counter drug for arthritis). I have included diclofenac to the protocol.
- Schwartz, 2013 New Cancer Paradigm and New Treatment: The Example of METABLOC
Third layer is my recommendation of many different supplements, based on my own research, especially based on results of Keith Block’s HALIFAX study and 3rd layer is also including James Morré EGCG protocol.
Keith Block and 180 other scientists wrote an in depth overview of cancers identifying 74 important targets in 11 main areas.
- Halifax study Keith Block article: Designing a broad-spectrum integrative approach for cancer prevention and treatment
- Morré, 2014. Cancer prevention trial of a synergistic mixture of green tea concentrate plus Capsicum (CAPSOL-T) in a random population of subjects ages 40-84
Main outcome
The main goal of this protocol is to block as many metabolic pathways used by cancer cells as possible – at the same time. This is the most important part – at the same time – to make it utmost difficult for cancer to re-adjust, re-route and develop resistance.
The desired result is to stop cancer from spreading and growing, to hibernate it – thus prolonging patient survival. Be aware, this is purely theoretical as we still don’t have any clinical study which would support this claim (first results of NCT02201381 testing COC part of the protocol will be no sooner than 2023).
All other positive outcomes will be bonus and we can just hope for them to happen. Like hoping that body can start fighting off the weakened cancer cells on its own. We don’t know what will / can happen.
Dosage and time of use
Orange color is COC protocol = metformin, atorvastatin, doxycycline and mebendazole. COC is one of the core part of the protocol. They are to be used daily.
All other supplements are to be used 3 days in a row with 4 days pause.
This is my preliminary suggestion – all depends on how demanding will the protocol be for kidneys and liver – so if you do tests every 4 weeks and all is good, you can possibly adjust the schedule to 4 to 3, or even to 6 to 1.
I am considering recommending using Morré and Schwartz sub-protocols also on a daily basis.
The lenght of the protocol is set to 3 months. After this, you should evaluate based on result of blood tests, PET, CT etc.
Dosage of supplements are approximate for cca 70kgs adult person.
If you plan a surgery
It is very important to note, that the protocol should be stopped at least 2 weeks prior to undergoing surgery, to avoid prolonged bleeding time or excessive blood loss during surgery (as some supplements in the protocol have anticoagulant effects). Always inform your doctor (anesthesiologist) about ALL supplements you take as soon as you know you are going to surgery and stop them in time, as it would be immensely difficult to evaluate potential effects for the anesthesiologist if you inform him/her late or stop the supplements late.
Who is suitable for the protocol?
The full protocol is not suitable for usage during conventional treatment. The reason is easy. We cannot estimate the interactions between all the drugs and supplements.
Therefore, the right time for this protocol is either before standard treatment (stop it at least 3 days before beginning of the treatment) or after the treatment (keep at least 48 hours time window).
There might be possibility to include at least COC or some specific supplements even during the standard treatment, but this needs to be evaluated on case to case basis, depending on what drugs patient takes and what oncological drugs are going to be used – many factors there to be considered.
If you intend to take this protocol for a long run, it is necessary to keep monitoring your kidneys and liver markers, and some other values as well (glucose, cholesterol etc.). Once in a month would be wise to have a check-up (blood test done) – to have feedback on how your body is reacting to all the pills. More details can be found in later section: What blood values to monitor during the protocol?
Tailoring the protocol ingredients
It should be possible, as cancers differ in metabolic profiles and differ also depending on what stage they are in. The future of anti-cancer treatments lies in tailoring the treatment for a specific patient.
Though, it is very difficult to do right now. My protocol here is as much universal as it can be. But when tailored, there may be some supplements added, some removed, and also dosage ratio can be adjusted (some supplements can be favoured more, and some less).
But frankly, even if we do our best, based on our current knowledge (which is very limited), it will still be more like a jump into the dark.
I believe the real true tailoring will be possible only after Artificial Intelligence/neural networks take over the cancer treatment – it will happen probably in about 10 years. As there are so many variables – humanoids simply cannot process and do the math. The tailored protocol these days would be just “best efforts” and “best guesses”.
Still first step would be to even try to map a metabolic landscape of a certain cancer. You can check for inspiration in Giunchi, 2018 The Metabolic Landscape of Prostate Cancer.
Ingredients of the protocol
RED zone – bio boosters
Bioperine
Commercial name for piperine. It is an extract from black pepper. It blocks some enzymes in liver. Blockage is causing better bioavailability of many supplements (more get into blood stream, less is metabolised in the liver out of body). We can call piperine a bio booster or a bio enhancer (helping to increase other substances bioavailability).
Half life of piperine (when half of the dose is still in the body) is 18 hours. The highest peak amount is after about 6 hours from ingestion. Therefore I put it on the very first spot in the morning in the protocol, to positively influence all other supplements taken later during the day. As a bonus, piperine shows interesting wide spectrum of anti-tumor effects on its own.
Two main ways how piperine enhances absorption is by inhibiting human P-glycoprotein and cytochrome CYP3A4. Both the proteins contribute to a major extent to first-pass elimination of many drugs (which we want to avoid). More in Gupta, 2013.
P–glycoprotein is a plasma membrane protein which acts as a localized drug transport, actively exporting drugs out of the cell. The inhibition of p-glycoprotein in cancer cells can theoretically mean they are not able to spit out what they don’t like. More of a drug stays in the cells.
More info
- Stojanovic-Radic, 2019. Piperine-A Major Principle of Black Pepper: A Review of Its Bioactivity and Studies
- P–glycoprotein inhibition can also help some drugs to cross blood-brain barrier. E.g. paclitaxel (Kemper, 2003)
Be careful about
- Avoid piperine during chemotherapy as:
- Piperine can influence metabolism of many drugs, especially those metabolised by CYP3A4 (includes more than 50% of drugs on market) and p-glycoprotein (P-gp) = it has high risk of drug interactions
- If you are using cannabis, be aware that piperine boosts both THC and CBD. For THC it is 3 fold increase in maximum serum concentration, for CBD it is 4 fold. Interesting to note for those who are on Rick Simpson protocol.
- If you take piperine for the very first time, try it alone and wait about 1 hour. It might cause stomach pain in some people, especially if they have gall bladder problems.
Products
Source Naturals 120 tablet (iHerb) 10mg in a capsule.
Swanson 60 capsules 10mg in a capsule.
You can buy it in bulk as powder and fill in your capsules, but it requires a sensitive digital scale, as the amount is very low and you should be careful and precise with dosing.
Quercetin
In the protocol quercetin is used as a second main bio booster (next to piperine). It increases absorption of many other substances like EGCG and Curcumin. The form of quercetine dihydrate has the best bioavailability. Quercetin may be quite powerful not only as a booster, but also in its own anti-cancer effects plus it also has a lot of synergies with other substances like curcumin and EGCG.
I consider quercetin in top 10 of natural dietary supplements in cancers.
Be careful with interactions. Quercetin influences drugs which are metabolised by CYP3A4, CYP2C8 and CYP2C19 enzymes. Also should not be mixed with chinolon antibiotics.
More info
- CancerTreatmentsResearch article: Quercetin: even more anti-cancer potential than Curcumin?
- Memorial Sloan Kettering article
- Reyes-Farias, 2019. The Anti-Cancer Effect of Quercetin: Molecular Implications in Cancer Metabolism
- Asemi, 2019. Quercetin: a natural compound for ovarian cancer treatment
Be careful about
- Avoid quercetin during chemotherapy as:
- Quercetin can influence metabolism of many drugs. Do not combine e.g. with taxane chemotherapy, dacarbazin, tamoxifen, anastrozol, exemestan, letrozole, erlotinib etc.
- AHFS Drug Information (2010) identifies quercetin as an inhibitor of CYP2C8, and specifically names it as a drug with potential to have harmful interactions with taxol/paclitaxel. As paclitaxel is metabolized primarily by CYP2C8, its bioavailability may be increased unpredictably, potentially leading to harmful side-effects.
- Possible risk groups. Quercetin may not be suitable for estrogen dependent tumor types and patients with pre-damaged kidneys. Also it is not possible to use together with certain medications (Andres, 2017).
Consider
- To use as pre-treatment before radiotherapy (together with melatonin and curcumin). Take 2-3 hours before the treatment to reach the peak blood levels during the treatment.
Lin, 2012. Combination of quercetin with radiotherapy enhances tumor radiosensitivity in vitro and in vivo.
Brito, 2015. Quercetin in Cancer Treatment, Alone or in Combination with Conventional Therapeutics? - Ovarian cancer Vafadar, 2020. Quercetin and cancer: new insights into its therapeutic effects on ovarian cancer cells
Products
I recommend to buy in a powder form (much cheaper then capsuled): Bulk Supplements. You can get cheap empty capsules on iHerb.
In capsules, you can buy on iHerb
Now Foods 240 capsules, 400mg of quercetin with little amount of bromelain (may help increase absorption).
Swanson 240 capsules with 250mg of quercetin + bromelain.
YELLOW zone – curcumin and synergistic ingredients
Curcumin
It is important to use curcumin with food or shortly after. Best with a fatty meal as it is a fat soluble substance.
Turmeric vs Curcumin. Curcumin is a naturally-occurring chemical compound found in the spice turmeric. Turmeric is the root of a plant which is scientifically known as Curcuma Longa and that’s probably where curcumin gets its name from. There is about 3% of curcumin in turmeric. In short, turmeric is something what you will use when cooking, curcumin is something you will use as a treatment.
When you want to enjoy benefits of turmeric when cooking food, add it at the end as the curcumin content lowers 24-53% when cooked for 10 mins (Suresh, 2007)
Curcumin has synergical effect with AKBA (Toden, 2015 a Zhi, 2011), EGCG (Kfafif, 1999; Angelo, 2010; Kondo, 2013 etc.), resveratrol (pterostilbene) and quercetin (Zhang, 2015) at this protocol.
There are so many studies with curcumin (Google Scholar), I will mention just a few (but please note, it seems to be clear so far, that curcumin is super potential in fighting cancers, but it has no chance on its own; we need group of heroes, one yellow-orange hero is not enough). But it is definitely one of the TOP 10 supplements you can take. Just it needs help of other supplements to do the work.
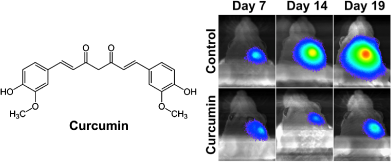
- Kim, 2015. Real‐Time Imaging Reveals Glioblastoma Suppression Effects of Curcumin in Mouse Brains
- Stigliano, 2015. Synergy with docetaxel. Mouse model. After 22 days of treatment, the combinatorial approach leads to complete disease regression. At 90 days post‐treatment initiation, mice injected with DTXL + CURC SPNs have a 100% survival, whereas only 50% of the DTXL SPN treated mice survive.
- YouTube video Aggarwal
- Lowers PSA levels in prostate cancer (Gupta, 2013)
- List of clinical trials with curcumin
For comprehensive summary check article on examine.com.
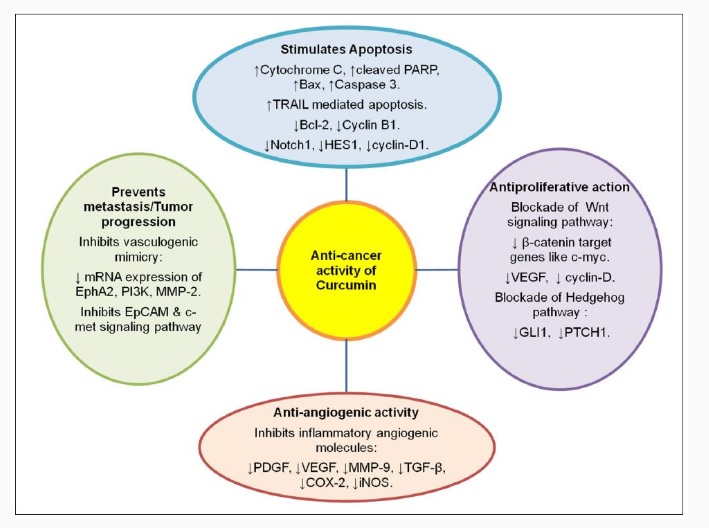
Check above some of the anti cancer effects of curcumin (source).

Consider
- To use as pre-treatment before radiotherapy (together with melatonin and quercetin). Take 1-2 hours before the treatment to reach the peak blood levels during the treatment.
- It should be safe to add with docetaxel (link) and gemcitabine (link; link).
Be careful about
- Orlowski, 2002. Dietary curcumin inhibits chemotherapy-induced apoptosis in models of human breast cancer.
It is necessary to carefully evaluate all supplements you want to use during chemotherapy. Some will be beneficial, some harmful, depending on what chemotherapy drug(s) you are given. Curcumin may work fine with some drugs, but not with all. - Patients with gastrointestinal disorders and those predisposed to kidney stone formation (Tang, 2008) should consult their physicians before using turmeric supplements.
- Also consult with doctor if you are on warfarin or other blood thinners.
- High dose of curcumin can change metabolism of many drugs, for example tacolimus. See in more details in Memorial Sloan Kettering article link.
- Monitor iron values, as similar to Alpha Lipoic Acid, long term curcumin therapy can lead to decrease of iron (Jiao, 2009).
Products
Very difficult to evaluate which curcumin is the best in price to content ratio. But it is clear that curcumin on its own has extremely low bio-availability (how much of the drug reaches blood circulation). So even 4 grams of curcumin, without any bio booster, can have almost no effect. So it is absolutely necessary to choose correct curcumin product. In this protocol, I have decided to go with piperine, as curcumin bio booster, based on Shoba, 1998. Piperine increased absorption about 20x times in humans.
Latest on bioavailability in Ghidoni, 2019. I am hoping that not only piperine, but other substances will help curcumin bioavailability in this protocol as well.
Don’t get tricked. Turmeric root extract contains only about 3% of curcuminoids. You want an extract standardised to 95% of curcuminoids. And you want to avoid “proprietary blends” when ratio of tumeric to curcuminoids extract is not stated.
For the protocol, we want curcumin without piperine, as we are supplementing piperine on its own therefore we need to avoid overdosing it. So the options are:
Theracurmin Swanson. About 11 USD per 30 caps/200mg. Turmeric Root Extract (Curcuma longa) (standardized to minimum 27% Theracurmin® curcumin)
Turmeric Phytosome with Meriva. About 11 USD per 60 caps/500mg. Meriva® Turmeric Phytosome™ (Curcuma longa rhizome/Glycine max soybeans) (standardized to 18–22% curcuminoids)
Now Foods Curcumin. About 26 USD. 120 caps / 665mg. Turmeric Root Extract (Curcuma longa) [Standardized to min. 95% Curcuminoids (630 mg) (including Curcumin, Demethoxycurcumin and Bisdemethoxycurcumin)]
Note, you would normally never buy product like this, as it has no added bio absorption enhancer, but we are taking Bioperine on its own, which is the only way to make this product work.
Jarrow Curcumin. About 22 USD. 120 caps / 500mg. Turmeric Extract (Curcuma C³ Complex®) (Curcuma longa) (95% [475 mg] Total Curcuminoids) (Rhizome)
For the time being, I will conside Now Foods as the top choice, as we will increase bio availability by piperine (which is old fashioned, but still the best choice in price to value ratio; Shoba, 1998).
Other different forms of curcumin may have better availability than curcumin+piperine combo, but the total amount in the capsule is much lower and the products are more expensive. So do the math. Even if I have 100% bio availability, but only 20mg of curcumin per capsule for 1 USD, I would rather buy 20% bio availability, with 400mg of curcumin per capsule for 30 cents.
Silymarin (Milk Thistle)
Added because of synergy with curcumin (increasing effectiveness of each other; Montgomery, 2016) and it has also synergy with berberine (Fogacci, 2019).
Moreover silymarin extract is great for liver health.
Last, but not least, it is a very promising substance against cancer stem cells (CSC) (Kumar, 2014; Raina, 2016). CSC should become one of the most important targets in cancers.
More info
- Reductions in liver toxicity with ALL chemotherapy. Ladas, 2009. A randomized, controlled, double‐blind, pilot study of milk thistle for the treatment of hepatotoxicity in childhood acute lymphoblastic leukemia (ALL)
- Anti-metastatic effects. Deep, 2010. Anti-metastatic Efficacy of Silibinin: Molecular Mechanisms and Therapeutic Potential against Cancer
- Examine.com article
Be careful about
- it is unclear whether and how Milk Thistle affects hormone driven cancers fueled by estrogen, so as a precaution you might avoid Milk Thistle for estrogen-based cancers. Alternatively, use only seeds extract of the plant as the seeds are supposed to show the lowest estrogen-like activity.
Products
iHerb Now Foods 200 capsules, 300mg. Product has 300mg of extract in a capsule plus little bit of dandelion and artychoke powder, which can add to positive liver health effect.
Alternatives Swanson 120 capsules 250mg of extract + 250mg of seeds.
AKBA (acetyl-11-keto-B-boswellic acid)
Detailed info in this article (only in Czech). AKBA has synergy with curcumin (Toden, 2014). It has important anti-inflammatory effect.
Important to use with food or shortly after, as it will have up to 5 times better absorption (link).
More info
- Roy, 2019. An Update on Pharmacological Potential of Boswellic Acids against Chronic Diseases
Tip for tailoring
- increase protocol dose for pancreatic cancer and brain cancers
Dosage
- Kinmatkar, 2013 patients used 333mg per capsule 3 times a day, but they used wide spectrum extract standardised to 45% of boswellic acids. In the protocol, we use an extract of one specific boswellic acid, which is called AKBA. Therefore we have 3 capsules a day only with 100mg per capsule. Sengupta, 2008 used 250mg 5-Lox extract per day for 90 days, without any side effects.
Products
iHerb ApresFlex Life Extension, 100mg (20% AKBA), 60 capsules.
Vitacost ApresFlex, 100mg (20% AKBA), 120 capsules.
Swanson Boswellia Serrata Extract 5-Loxin, 125mg (30% AKBA), 60 capsules.
Berberine
One of the most promising substances, which shows synergy with curcumin (Wang, 2016), silymarin (Fogacci, 2019) and melatonin (Lu, 2016). I wrote a short article about it (in Czech). It interferes with metabolic processes in cancer cells, especially metabolism of glucose. It is similar to Metformin, but not the same, it complements it (Wang, 2018).
I consider berberine to be between TOP 10 supplements you can use in cancers.
Piperine and Milk Thistle helps the bio availability of berberine by inhibiting its efflux by p-Glycoprotein.
In the protocol, it is added after meal. I haven’t found any reason why it should be taken before meal (if we take it against cancer). By taking it after, we can avoid possible stomach pain.
More info
- Comprehensive information on berberine can be found in examine.com article.
- Self-hacked article
- Xu, 2019. Anticancer effect of berberine based on experimental animal models of various cancers: a systematic review and meta-analysis
“BBR exerted anti-tumor effects in a variety of tumors in vivo, especially breast cancer and lung cancer, and the evidence was still insufficient in colorectal cancer and gastric cancer.” - Chen, 2020. Berberine versus placebo for the prevention of recurrence of colorectal adenoma: a multicentre, double-blinded, randomised controlled study.
“Berberine 0,3 g twice daily was safe and effective in reducing the risk of recurrence of colorectal adenoma and could be an option for chemoprevention after polypectomy.”
Be careful about
- does influence CYP2D6, CYP2C9 and CYP3A4, so you need to be careful when taking drugs metabolised by these
- do not use together with microlide antibiotics such as azithromycin and clarithromycin (may lead to serious cardiotoxicity)
- do not use after brain injury
Dosage
- We have 3 caps per day, each 400mg. Most trials were in range of 0.5-1.5g per day.
Products
Berberine in capsules is quite expensive. I would recommend buying powder in bulk and capsule on your own. It is not possible to just dilute in water, as it is very bitter.
BulkSupplements powder.
Swanson 60 capsules 400mg.
Honokiol
Wikipedia Honokiol article.
- Honokiol helps to increase efficacy of curcumin (Srivastava, 2007)
- Pan, 2016: “Honokiol targets mitochondria to halt cancer progression and metastasis.”
- Rauf, 2018: “Honokiol: An anticancer lignan.”
- PTEN activation (Liu, 2008)
- STAT3 inhibition Kumar, 2013
Dosage
- We have 3 caps per day for 200mg.
Sarrica, 2018. Safety and Toxicology of Magnolol and Honokiol.
Examine.com article.
Products
Swanson 30 capsules. 90% honokiol.
NutriCology Innovative Nutrition. Magnolia Extract Honokiol + Magnolol 90%. 120 caps 200mg.
VIOLET zone – Laurent Schwartz METABLOC protocol
Alpha Lipoic Acid will try to block PDK (pyruvate dehydrogenase kinase) production by cancer cells, thus to block them possibility to make lactate from pyruvate.
Diclofenac will block lactate transporters, thus blocking export of lactate in and out of cancer cells.
Cancer cells are trying to put all the excessive amount of lactate out and by blocking it, we are trying to make them fed up with their own lactate production (also atorvastatin helps in this sense see Leung, 2017).
Lactate is a multi-purpose weapon of cancers. By spreading it around themselves they are trying to expand and protect themselves at the same time – poisoning their surroundings with lactate lowers pH (which can lead to easier metastasis formation Gort, 2008) and it also makes it difficult for human immune cells to work at such polluted environment (Choi, 2013; Haas, 2015). The reason is that e.g. T Cells are using glycolysis as well thus they are producing lactate on their own as a waste metabolite. But when environment is overloaded with lactate, they have problem to unload it.
Fisher, 2007 showed that when there is a lactic acid present, it suppresses the proliferation and cytokine (signalling messangers) production of human cytotoxic T lymphocytes (CTLs) up to 95% and leads to a 50% decrease in cytotoxic activity.
Recap – utmost important role of lactate in cancers
- Lactate tossed out of cancer cells is making neighborhood toxic for immune cells (they cannot unload their own waste)
- Lactate shield. Lactate has anti-oxidant abilities and is used against anti-cancer drugs, shielding them against damage (Groussard, 2000)
- Lactate makes neighborhood acidic, which makes spreading easier (Gort, 2008)
- Lactate is used by cancers to buy loyalty from fibroblasts, to bribe them (CAFs – Cancer Associated Fibroblasts). Cancer pays a lactate coin and in exchange, fibroblasts help cancer to migrate into surroundings (Rattigan, 2012)
- Not only that. Those treacherous CAFs are, for a measly lactate coin, helping cancer cells to defend against chemotherapy, by producing protein WNT16B for them (Johnson, 2013).
Alpha Lipoic Acid (ALA)
Take before meal (about +20% absorption improvement), 3 times a day, 600mg per dose. Comprehensive summary in Examine.com article.
- Berkson, 2009. Revisiting the ALA/N (α-Lipoic Acid/Low-Dose Naltrexone) Protocol for People With Metastatic and Nonmetastatic Pancreatic Cancer: A Report of 3 New Cases
- Baronzio, 2010. Adding a combination of hydroxycitrate and lipoic acid (METABLOC TM) to chemotherapy improves effectiveness against tumor development: Experimental results and case report
- Sutendra, 2013 Pyruvate dehydrogenase kinase as a novel therapeutic target in oncology.
- Schwartz, 2013. New Cancer Paradigm and New Treatment: The Example of METABLOC
- Schwartz, 2014. Metabolic Treatment of Cancer: Intermediate Results of a Prospective Case Series
- Berkson, 2017. The Long-Term Survival of a Patient With Stage IV Renal Cell Carcinoma Following an Integrative Treatment Approach Including the Intravenous α-Lipoic Acid/Low-Dose Naltrexone Protocol
- Schwartz, 2017. Out of Warburg Effect: an effective cancer treatment targeting the tumor specific metabolism and dysregulated pH
- Peres, 2019. Metabolic therapies inhibit tumor growth in vivo and in silico.
Be careful about
- Do not confuse with ALA as Alpha-Linolenic Acid
- Monitor iron levels during long term ALA therapy, as ALA may chelate it out of body
Note
- On market you can find Alpha Lipoic Acid and R-Alpha Lipoic Acid. The latter is much more expensive, claiming superiority over the normal one. While it may have better bio availability, the difference is not substantial enough to be worth the extra money. All the lenghty texts about it on internet are just for marketing-lies.
So save the pennies (and better toss a coin to your Witcher – O’ Valley of Plenty).
Hydroxycitric Acid (HCA)
HCA (extract from Garcinia Cambogia) inhibits ACLY, which in result inhibits fatty acid synthesis from carbohydrates. HCA is very unique as there are not many other substance targeting ACLY with almost no toxicity (compare to Bempedoic Acid article).
Zaidi, 2012 “ACLY is cross-link between Glucose and/or Glutamine Metabolism and Fatty Acid Synthesis and/or Mevalonate Pathways”.
Also note “Cancer cells displaying a high rate of glucose metabolism are more severely affected by ACLY inhibition.” (Zhao, 2005).
ACLY is discussed later in the article in more details.
Take with ALA, before meal, 3 times a day. 500mg a dose.
- Zu, 2012 ATP Citrate Lyase Inhibitors as Novel Cancer Therapeutic Agents
- Migita, 2014 Inhibition of ATP citrate lyase induces triglyceride accumulation with altered fatty acid composition in cancer cells
- Wen, 2019. ACLY facilitates colon cancer cell metastasis by CTNNB1
- Span, 2019. ACLY (ATP Citrate Lyase) Mediates Radioresistance in Head and Neck Squamous Cell Carcinomas and is a Novel Predictive Radiotherapy Biomarker
Diclofenac
Dosage to be reviewed. Preliminary, I would suggest to take one pill (25mg) every third day with the morning dose of ALA/HCA.
Diclofenac serves as important blockator of lactate transporters MCT1 and MCT4. Lactate is the end product of glycolysis, often considered as waste metabolite, but cancers can make good use of lactate to modify the landscape around them. Several tumors and inflammatory sites show accumulation of lactate and altered expression of its transporters, thus suggesting a role of this metabolite in cancer and inflammation.
Diclofenac also inhibits LDH-A (lactate dehydrogenase; Leidgens, 2015).
- Pantziarka, 2016. Repurposing Drugs in Oncology (ReDO) – diclofenac as an anti-cancer agent
- Renner, 2019. Restricting Glycolysis Preserves T Cell Effector
Functions and Augments Checkpoint Therapy
Be careful about
- We need to take into consideration when setting proper dose of diclofenac that piperine can boost diclofenac bio availability about +150%
The below graphs from Peres, 2019 are showing how important is to use more supplements at the same time. In mice, the METABLOC worked only with high dose metformin and even better with high dose metformin and high dose diclofenac.

Products
iHerb Health Origins ALA 150 capsules 600mg.
iHerb Now Foods HCA 120 capsules 500mg.
Diclofenac is available over the counter in pharmacy.
GREEN zone – D. James Morré protocol
EGCG
Taking EGCG + quercetin + cayenne is based on anti-cancer protocol invented by James Morré (Morré, 2003; Morré, 2014).
The original Morré protocol is suggesting to take EGCG every 4 hours, 6 times a day, but this is extremely inconvenient though it has its merits (you can find explanation in articles above).
Also it is very important to really add capsaicin (in form of chili guajillo), otherwise you will lose a lot of cancer-killing power. Citing from Morré: “Additionally, a product containing a synergistic combination of decaffeinated green tea and a commercially available vanilloid-containing Capsicum preparation at a ratio of 25:1, resulted in a 100 fold increase in killing of cultured cancer cell lines compared to green tea alone.”
It aims to eliminate ENOX2 proteins from blood stream, thus reducing metastatic potential of cancers. It is important to take EGCG before food, as the bioavailability is much better as published in Naumovski, 2015.

EGCG goes well with
- Quercetin Wang, 2012; Prawan, 2014; Srivastava, 2010; Wang, 2015. 2-4 times increase of bioavailabity + 4-10 times increase of EGCG concentration in cancer cells.
- Piperine. Mereles, 2011 increasing bioavailability of EGCG
- Luteolin. Gray, 2014; Amin, 2010; Wu, 2014
- Cayenne. Morré, 2003, Morré, 2014
More info
- Khan, 2011. Cancer and metastasis: prevention and treatment by green tea
- Rady, 2017. Cancer preventive and therapeutic effects of EGCG, the major polyphenol in green tea
Be careful about
- long term usage (for many months) of EGCG can influence CYP3A4 levels even for many weeks after you quit EGCG. This can rarely happen also with very strong regular green tea drinkers. Keep this in mind if you ever plan to undergo operation with anesthesia and inform doctors. Meaning, if you take EGCG for a very long time, it can theoretically influence CYP3A4 levels and it can take weeks after you quit to reach normal levels. Long term EGCG usage can thus increase/decrease blood levels of many different drugs e.g. tamoxifen, irinotecan, verapamil, acetaminophen and many others which are metabolised by CYP3A4.
- do not take with bortezomib Golden, 2009
- avoid EGCG when having liver disease (alternatively, close monitoring is required)
- avoid when having kidney disease (alternatively, close monitoring is required)
Products
iHerb Life Extension 100 capsules. 326mg EGCG in a capsule. I choose this one as it has optimal amount in 1 capsule. Alternative is Now Foods product, but with only 200mg.
There is a patented product called Capsol T, with unknown relation to Morré himself. I do not recommend to buy it, because it is very expensive (150 USD for 180 caps). Moreover, it contains only EGCG and chilli extracts, not quercetin. But quercetin is very important for bio absorption of EGCG as well.
Chilli Guajillo
- Instead of Cayenne extract, which may be too agressive for some people stomach, you can buy Chilli Guajillo which have only between 2500 to 8000 Scoville units. So they are very mild. Both would work. Actually, original Morré protocol has Guajillo used.
- I tested cayenne extracts, but even if it has 40000 Scoville units, it may be painful for stomach (and I like chilli). Some products are even with 90000+ Scoville units.
BLUE zone – The Magnificent Five
Holy Basil (oleanic acid, ursolic acid)
Holy Basic is a source of oleanic acid and ursolic acid.
- Gajula, 2010. Basil (Ocimum basilicum and Ocimum tenuiflorum) Reduces Azoxymethane Induced Colon Tumors in Fisher 344 Male Rats
- Batra, 2013. Holy Basil leaf extract decreases tumorigenicity and metastasis of aggressive human pancreatic cancer cells in vitro and in vivo: Potential role in therapy
- Liu, 2014, Oleanolic acid induces metabolic adaptation in cancer cells by activating the AMP-activated protein kinase pathway.
- Žiberna, 2017. Oleanolic Acid Alters Multiple Cell Signaling Pathways: Implication in Cancer Prevention and Therapy
- Iqbal, 2018. Ursolic acid a promising candidate in the therapeutics of breast cancer: Current status and future implications
Be careful about
- do not use during radiation therapy
Products
iHerb Himalaya 60 capsules. 500mg 0.4% Ursolic acid and Oleanolic acid, 2.0 mg + 60mg Holy Basil supercritical CO2 extract 2.5% Ursolic acid and Oleanolic acid, 1.5 mg)
Swanson Now Foods 90 capsules 500mg min. 2% ursolic acid.
Vitacost 180 capsules, 400mg min. 2% ursolic acid.
Pterostilbene
Pterostilbene is an analog of resveratrol (they differ by a single element) which is much better absorbed than resveratrol. Therefore I have used it instead of the much better known resveratrol. There is much more studies about resveratrol, but pterostilbene is very similar and have much better bioavailability.
Pterostilbene has synergy with tocotrienols (Sylvester, 2017), with melatonin (Jung, 2019), with quercetin (Ferrer, 2005) and probably also other substances which have proven synergy with its cousing resveratrol. In melanoma you can add pterostilbene + inositol to the protocol (Schneider, 2009).
Optional suggestion
There is a possibility to attempt for synergy and add also a morning 1 capsule of 500mg of resveratrol (product) and to take it together with a morning dose of piperine, as Johnson, 2011 found the big increase in bioavailability of resveratrol (but compare to Bailey, 2020, who found no effect – though they used only a single dose, which may be not enough to block enzymes – and also you need to pre-treat with piperine, not to take simultaneously).
- Xing, 2016. Abstract 905: Pterostilbene (PTER) suppresses breast cancer brain metastasis by targeting a c-Met mediated inflammation network
- Benlloch, 2016. Pterostilbene Decreases the Antioxidant Defenses of Aggressive Cancer Cells In Vivo: A Physiological Glucocorticoids- and Nrf2-Dependent Mechanism
- Chan, 2019. Resveratrol and pterostilbene: A comparative overview of their chemistry, biosynthesis, plant sources and pharmacological properties
- Shin, 2020. Pterostilbene Suppresses both Cancer Cells and Cancer Stem-Like Cells in Cervical Cancer with Superior Bioavailability to Resveratrol
More info
- A bit older Life Extension article from 2009 “The “Other” Resveratrol”
- Examine.com article
Products
Swanson 30 capsules, 50mg.
Jarrow Formulas 60 caps, 50mg.
Apigenin
Apigenin and Luteolin are “Flavones Brothers”. Flavones (flavus = yellow), are a class of flavonoids.
Apigenin goes well with EGCG Hoensch, 2008 and with curcumin Choudhury, 2013.
Check potential of synergy with paclitaxel (Xu, 2012); doxorubicin (Korga, 2019); 5-FU (Hu, 2014).
More info
- LifeExtension article on Apigenin
- Examine.com article
- Shukla, 2010 Apigenin: A Promising Molecule for Cancer Prevention
- Srivastava, 2010 Antiproliferative and Apoptotic Effects of Chamomile Extract in Various Human Cancer Cells
- Bilirale, 2016. The flavonoid apigenin reduces prostate cancer CD44(+) stem cell survival and migration through PI3K/Akt/NF-κB signaling.
- Yan, 2017. Apigenin in cancer therapy: anti-cancer effects and mechanisms of action
- Salehi, 2019. The Therapeutic Potential of Apigenin
Be careful about
- Don’t use Apigenin when on hormone replacement therapy with a progestin (2013; though compare with 2012)
Products
Swanson 90 capsules 50mg.
We may need quite high dose of Apigenin to have effect (Abel, 2016). You have 1 bottle for 15 days if taken 6 times a day. To reduce costs, we may opt for BulkSupplements Chamomille extract in powder. Would it have comparable effect? How much would you need to take to get equivalent of 50mg of apigenin?
Some sources say a standard extract has about 1,2% of apigenin. And one cup of chamomile tea has up to 9,3mg of apigenin (link). In the protocol I recommend to take at least 300mg a day (6x50mg), so it would not be feasible just by drinking tea and would be pretty difficult even if having the extract with 1,2%. So here, I guess we would need to stick with the pure apigenin extract.
Luteolin
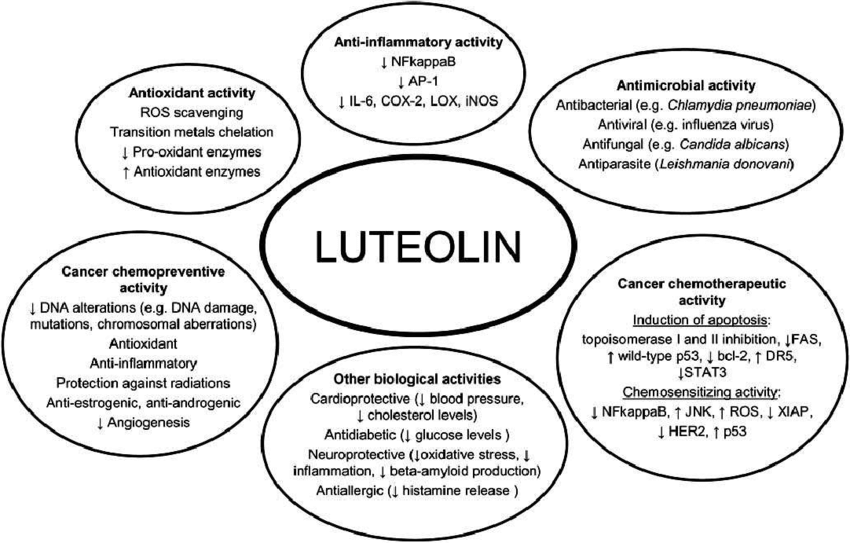
More info
- SelfHacked article
- Tuorkey, 2016. Molecular targets of luteolin in cancer
- Wang, 2018. Luteolin: Anti-breast Cancer Effects and Mechanisms
- Imran, 2019. Luteolin, a flavonoid, as an anticancer agent: A review
Tips for tailoring
- with cisplatin for ovarian cancer (Wang, 2018). Though note there is in vitro study with oxaliplatin colorectal carcinoma cells which has a different outcome (Jang, 2019). It is related to Nrf2, I wrote an article about it in Czech and the complex foggy situation around Nrf2 activators led me to exclude Broccoli extract (Sulphoraphane) from the protocol as Sulphoraphane is a strong activator of Nrf2.
- in general, as luteolin is inhibitor of Nrf2, it should be beneficial to use together with chemotherapy, especially in advanced cancers, but I suggest to study this on case to case basis.
Products
Swanson 30 capsules; 50mg.
The supplement is very expensive, as we may need quite high dose of Luteolin to have effect (Abel, 2016). One bottle will be only for 5 days (if 6 caps are taken per day).
Maybe BulkSupplements Parsley Extract may work instead? As parsley is high in both apigenin and luteolin so it seems to be a good choice. For info check flavones content in vegetables.
Other high sources of flavones – use when cooking:
- Mexican dried Oregano
- Thyme, Rosemary
- Artichokes
- Parsley
- Radicchio
- Celery / celery seeds
Fisetin
Fisetin is commonly found flavonoid in strawberry, apple, persimmon, kiwi, peach, grapes and onion . The highest concentration is reported in strawberries (160 μg/g) followed by apple (26.9 μg/g) and persimmons (10.5 μg/g).
- May work well with Cisplatin. Shaha, 2011. Anticancer Activity of a Combination of Cisplatin and Fisetin in Embryonal Carcinoma Cells and Xenograft Tumors
May work well with 5-FU. Khan, 2019. Fisetin and 5‐fluorouracil: Effective combination for PIK3CA‐mutant colorectal cancer - Wang, 2018. Anti-cancer effects of fisetin on mammary carcinoma cells via regulation of the PI3K/Akt/mTOR pathway: In vitro and in vivo studies
- Li, 2018. Fisetin Inhibited Growth and Metastasis of Triple-Negative Breast Cancer by Reversing Epithelial-to-Mesenchymal Transition via PTEN/Akt/GSK3β Signal Pathway
- Kashyap, 2019. Fisetin and Quercetin: Promising Flavonoids with Chemopreventive Potential
Be careful about
- might have inhibitory effect on CYP2C8 (e.g. paclitaxel), CYP2C9 and CYP2D6 (= can influence e.g. Tamoxifen). Also influences CYP2C19 and CYP1A2.
Products
Swanson 30 capsules 100mg.
Doctor’s Best 30 capsules, 100mg.
BROWN zone – tocotrienols + sesamine
Tocotrienols
There are two forms of vitamin E: tocotrienols and tocopherols. Unlike better known tocopherols, tocotrienols are displaying promising anticancer effects.
Important point
Must have only tocotrienols! Avoid mixing of tocopherols and tocotrienols as it weakens anti-cancer effects as proven in Shibata, 2010. Important point, completely ignored in existing protocols.
More info
- Hiura, 2009. Specific accumulation of gamma- and delta-tocotrienols in tumor and their antitumor effect in vivo.
- Synergy with docetaxel; atorvastatin, celecoxib, erlotinib, gefitinib (Bachwal, 2010)
- Synergy with bortezomib, thalidomid and gemcitabin (Ye, 2015; Husain, 2013)
- Husain, 2013. Vitamin E δ-tocotrienol prolongs survival in the LSL-KrasG12D/+;LSL-Trp53R172H/+;Pdx-1-Cre (KPC) transgenic mouse model of pancreatic cancer.
- Clinical study. Springett, 2015. A Phase I Safety, Pharmacokinetic, and Pharmacodynamic Presurgical Trial of Vitamin E δ-tocotrienol in Patients with Pancreatic Ductal Neoplasia
- Synergy with EGCG, resveratrol (Wu, 2008); with curcumin (Steuber, 2016; Nesaretnam, 2012, patent); with ginger root extract Yusof, 2015.
- Other info in Rosenthal, 2014; Aggarwal, 2010 and Ahsan, 2014.
Products
Swanson 60 capsules / 100mg. Product must have only tocotrienols. Avoid products mixtures of tocopherols and tocotrienols as it weakens anti-cancer effects.
Compare price with
Nutricology 125mg / 90 capsules (delta 90%, gamma 10%)
Nutricology 50mg / capsules (delta 90%, gamma 10%)
Current 3/4 version of the protocol would have 6 capsules a day. In 3 days it is 18 capsules. It is one of the most expensive supplement in the protocol.
Adjustment of the protocol in BROWN ZONE
I am considering an adjustment having tocotrienols only one time in a month, but for 7 continuous days, in mega dosage, following the Clinical study and trying to achieve the accumulation of tocotrienols in cancer cells, as suggested in Hiura, 2009:
“These results, to our knowledge, are the first demonstration of specific accumulation of gamma-T3 and delta-T3 in tumors and suggest that T3 accumulation is critical for the antitumor activities of T3.”
The suggested dosage would be 1600mg a day for 7 days (it would take 1 Nutricology 125mg 90caps bottle). Somehow, Hiura experiment showed that 1600mg has the maximum efficiency, even higher than 3200 mg, so we will stick to it.
Moreover, compared to Hiura, we will try to boost the bio availability by sesamine and piperine, hoping to achieve even much more substantial effect.
Tahini Sesame Paste
Tahini is a sesame seed paste. It is a source of sesamin which helps to increase bio availability of tocotrienols. It is very important as sesamine blocks degradation of tocotrienols and benefit may be even up to 500% (examine.com). There used to be supplements with sesamine extract, but they are discontinued. I can find some products, but I don’t have experience with the web sites, so be careful.
Lignans for Life. Product 90 caps, a caps has 81 mg of sesamin and 27 mg of sesamolin.
SesaPlex 100 mg. 30mg sesamin, 10mg sesamolin.
Tahini might be a sub optimal way to get sesamine, so I am open for suggestions (hoping one of the above supplements will work or any other source of sesamine from food?).
It is sub-optimal because of high copper content (I believe we should reduce copper intake in cancers) and some people may not like high content of omega 6 fatty acids (see content in 100 grams).
GREY zone – vitamin K2 + D3
Vitamin K2 + D3 combination is very powerful. Not only in anti-cancer effects, but the combination is good for bone health (e.g. it increases Bone Mineral Density – BMD).
- occasionally supplement magnesium as well, as it helps D3 metabolism (Uwitonze, 2018). Choose the proper form. Avoid cheap forms with very low bio-availability (under 5%) like magnesium oxide. A safe bet is to pick magnesium citrate.
The key is the combination as supplementing high dose D3 alone for long time can lead to decrease in BMD (Burt, 2019). But taking both can revert it (Ushiroyama, 2002; Je, 2011; Iwamoto, 2000; 2003; Frandsen, 2016; van Ballegooijen, 2017).
Vitamin K2 MK-4 (Menatetrenone; also called Menaquinone)
K vitamins are fat soluble. Use with food.
- Mizuta, 2006. The effect of menatetrenone, a vitamin K2 analog, on disease recurrence and survival in patients with hepatocellular carcinoma after curative treatment: a pilot study.
- Bullo, 2014. Dietary Intake of Vitamin K Is Inversely Associated with Mortality Risk.
- Synergy with sorafenib (Tae-Yong Ha, 2015; Jung, 2015)
- Fan XV, 2018. Research progress on the anticancer effects of vitamin K2.
- Reinan, 2018. Vitamin K and multiple diseases: a comparison between vitamin K1 and vitamin K2.
- Felix DiFara Life Extension article. The Remarkable Anticancer Properties of Vitamin K.
- Susan G. Komen website article
- Linus Pauling Institute article
- Comprehensive summary at examine.com
Be careful about
- avoid combination with Warfarin (Coumadin). Vitamin K is used by the body to help blood clot. Warfarin (Coumadin) is used to slow blood clotting. By helping the blood clot, vitamin K might decrease the effectiveness of warfarin. Be sure to have your blood checked regularly. The dose of your warfarin might need to be changed.
Products
iHerb Advanced Orthomolecular Research AOR 90 capsules. 15mg Menatetrenone MK-4 per capsule.
Carlson Labs, Vitamin K2, 5 mg Menatetrenone, 60 capsules.
Vitamin D3
Blood level should be kept within 50 to 100 ng/mL. Levels under 30 are resulting in worse survival. Important to note that most patients are having decifit which can be improved only by supplementation, especially during winter.
- Maalmi, 2014. Serum 25-hydroxyvitamin D levels and survival in colorectal and breast cancer patients: systematic review and meta-analysis of prospective cohort studies.
- Mohr, 2014. Meta-analysis of Vitamin D Sufficiency for Improving Survival of Patients with Breast Cancer
- Gorham, 2015. Could vitamin D sufficiency improve the survival of colorectal cancer patients?
- Wesa, 2015. Serum 25-hydroxy vitamin D and survival in advanced colorectal cancer: a retrospective analysis.
- Baron, 2015. A Trial of Calcium and Vitamin D for the Prevention of Colorectal Adenomas
- NG, 2019. Effect of High-Dose vs Standard-Dose Vitamin D3 Supplementation on Progression-Free Survival Among Patients With Advanced or Metastatic Colorectal Cancer: The SUNSHINE Randomized Clinical Trial.
More info
- If your lab report uses nmol/L, you can use converter to ng/mL
Safety concerns
The protocol uses 20000 IU per day. For 3 days a week, it is total of 60000 IU per week. I would recommend not to go over this weekly dose. So if you adjust the protocol to let’s say 4 days with 3 days pause, keep it equal/under 60000 IU. You can do regular quarterly or biannual tests for serum 25-hydroxyvitamin D levels.
- Jetty, 2016. Safety of 50,000-100,000 Units of Vitamin D3/Week in Vitamin D-Deficient, Hypercholesterolemic Patients with Reversible Statin Intolerance.
“Vitamin D3 therapy (50,000-100,000 IU/week) was safe and effective when given for 12 months to reverse statin intolerance in patients with vitamin D deficiency. Serum vitamin D rarely exceeded 100 ng/mL, never reached toxic levels”
- Avoid any calcium supplements during the protocol, as vitamin D3 increases calcium absorption from food. By supplementing it, you can put yourself in risk of too much calcium (hypercalcemia). I would also limit consumption of any high calcium food (examples).
- Be careful if you have a granulomatous disease such as sarcoidosis or tuberculosis and tumors such as lymphomas. Supplementation of D3 should probably be avoided completely. Though in lymphomas, it is worth to study deeper (e.g. Hohaus, 2018).
ORANGE zone – COC protocol
The COC Protocol when used alone is intended for use as an adjunctive therapy, meaning a therapy given in addition to the main treatment to maximize its effectiveness. As I wrote in the beginning, the whole “Full Metabolic Blockage of Cancer Cells Protocol” is not suitable to be used together with main treatment, because of too many possible interactions. But the COC alone, it has only 4 drugs and it is theoretically possible to assess risk/benefits and possible interactions. But it needs to be done on case to case basis.
Care Oncology Clinic main focus is currently on glioblastoma. They have made a retrospective study which is showing promising increase of median survival (see Agrawal, 2019 link below).
- COC Protocol in Glioma
- COC protocol for Blood Cancers
- COC protocol for Colorectal cancer
- Agrawal, 2019. A New Method for Ethical and Efficient Evidence Generation for Off-Label Medication Use in Oncology (A Case Study in Glioblastoma)
Interestingly, there is a curious attempt to treat cancer, which is sort of bizzare though, which share two of the drugs with COC (mebendazole and doxycyclin). You can check in details here NCT02366884 / Atavistic Chemotherapy.
Metformin
Drug prescribed worldwide to control hyperglycaemia. It has a very well-established safety profile. Gastrointestinal adverse effects (in particular at the beginning) are quite common, and often mild and manageable.
Start with 2x 500mg a day (first pill with breakfast, second with dinner). After 2 weeks, increase to 2x 1000mg a day (one 1000mg in the morning, another one in the evening).
Best bioavailability is when taken before food, but it depends on the form of metformin. Extended-release pills are better with food, normal pills without.
Citing from drugbank.ca:
“Food reduces the absorption of metformin, as demonstrated by about a 40% lower mean peak plasma concentration (Cmax), a 25% lower area under the plasma concentration versus time curve (AUC), and a 35-minute increase in time to peak plasma concentration (Tmax) after ingestion of an 850 mg tablet of metformin taken with food, compared to the same dose administered during fasting Label.
Though the extent of metformin absorption (measured by the area under the curve – AUC) from the metformin extended-release tablet is increased by about 50% when given with food, no effect of food on Cmax and Tmax of metformin is observed. High and low-fat meals exert similar effects on the pharmacokinetics of extended-release metformin.”
More info
- There is association between metformin and cancer mortality. The patients taking metformin survive longer (Zi, 2018; Saraei, 2019). The evidence is pretty solid. We may don’t know exactly why is it happening, but we know it is happening. This makes metformin very promising drug to add to anti-cancer coctail.
- Synergy of metformin with statins Wu, 2014; Nimako, 2017
- Consider strong synergy with Syrosingopine Benjamin, 2018
Be careful about
- In BRAF-driven melanoma, I suggest to increase the supplements which are inhibiting VEFG. Martin, 2012. Metformin Accelerates the Growth of BRAFV600E-Driven Melanoma by Upregulating VEGF-A.
- theoretical B12 deficiency as a result of taking metformin in discussed here
- You should have regular blood tests, with metformin focusing on renal values.
Safety concerns
- Be sure to read package leaflet to learn about all side effects, interactions and contraindications. You can also check it online at drugs.com.
- Lactic acidosis. A very rare dangerous side effect. You should learn about it, check e.g. Silvestre, 2019. Lactic acidosis is the reason why metformin is contraindicated for patients with renal impairment, as this is the main risk factor (plus age over 70, alcohol consumption and long term use of high dose over 3 grams).
Do not panic though as lactic acidosis is extremely rare. See DeFronzo, 2016: “However, the reported incidence of lactic acidosis in clinical practice has proved to be very low (< 10 cases per 100,000 patient-years).”
Atorvastatin
Widely prescribed to regulate high cholesterol since the 1990s. Most people tolerate atorvastatin well without any problems.
Dosage
40 mg a day. Start with half of this dose and after 2 weeks increase to the full dose.
Important. When following 3/4 protocol, use only 20mg a day on those days when you take all other supplements as well. Example Monday to Sunday 20/20/20/40/40/40/40. The reason is discussed in Safety Concerns below.
Be careful about
- Drug interaction with oxaliplatin (drugs.com)
- Monitor your blood levels for liver health markers (especially ALT and AST values).
Safety concerns
- Be sure to read package leaflet to learn about all side effects, interactions and contraindications. You can also check it online at drugs.com.
- Atorvastatin is influenced by CYP3A4 inhibitors (medsafe). Using the inhibitors will lead to increase of blood level of atorvastatin. This can increase the risk of side effects such as liver damage and a rare but serious condition called rhabdomyolysis that involves the breakdown of skeletal muscle tissue.
Protocol contains some CYP3A4 inhibitors (piperine is the strongest), so the daily dose during the days you take piperine should be decreased to 20mg, instead of 40.
Doxycycline
Tetracycline antibiotic has been used clinically for over 50 years. Common
adverse effects include gastrointestinal problems and photosensitivity. In cancer therapy, it has been recently used with cetuximab, as prevention of skin rashes (so not due to any anti-cancer effects).
Doxycycline 100 mg 1x/day.
Combination with vitamin C is suggested (De Francesco, 2017). If you supplement iron, take it at least 4 hours after doxycycline.
Doxycycline is switching with Mebendazole. 1 month doxycycline, second month mebendazole.
Be careful about
- Nanda, 2016. Doxycycline Promotes Carcinogenesis & Metastasis via Chronic Inflammatory Pathway: An In Vivo Approach
- Monitor your blood levels for liver health markers.
- Doxycycline negatively affects microflora of the gastrointestinal tract. I suggest to supplement probiotics after doxy, during the mebendazole month.
Study has researched the doxy alone on rats, it can be different in humans. In the protocol we have enough anti-inflammatory supplements to avoid chronic inflammation in colon. To rectify this theoretical negative side-effect of doxy.
Compare to Manna, 2018 as they found protective effect of doxy in rats. Therefore I would suggest we don’t need to be afraid here.
Safety concerns
- Be sure to read package leaflet to learn about all side effects, interactions and contraindications. You can also check it online at drugs.com.
- Doxycycline should be discontinued if significant diarrhea occurs during therapy as there might be a link with antibiotic therapy and colitis.
- Do not take isotretinoin (Accutane) and vitamin A during doxycycline therapy. Isotretinoin may be used as a chemotherapy (although it is normally used as a treatment for severe acne) to treat certain types of cancer such as neuroblastoma. There is risk of rare but very serious side effect with this combination.
Mebendazole
Commonly used to treat parasitic worm infections. It has low-toxicity.
Mebendazole 100 mg 1 time a day. Use always after meal. In the protocol, we take one month mebendazole, than one month doxycycline instead.
- To increase bio availability of Mebendazole, you can use cimetidine (Pirotte, 1987).
- Guerini, 2019. Mebendazole as a Candidate for Drug Repurposing in Oncology: An Extensive Review of Current Literature
- Bodhinayake, 2015. Interesting results in mice in meduloblastoma (children brain cancer). More in NCT02644291; NCT01729260; NCT01837862
Tips for tailoring
- Mebendazole have high potential for synergy with radiotherapy and with chemotherapy drugs. Do a quick search with your chemo drug.
- Zhang, 2018. Mebendazole Potentiates Radiation Therapy in Triple-Negative Breast Cancer
- Docetaxel (Rushworth, 2019)
- Temozolomide (Kipper, 2018)
Safety concerns
- Be sure to read package leaflet to learn about all side effects, interactions and contraindications. You can also check it online at drugs.com.
- Monitor your blood levels for liver health markers (especially ALT, AST and GGT values).
BLACK zone – Bedtime
Ashwagandha
- Comprehensive article on Examine.com and Memorial Sloan Kettering article
- SelfHacked article.
- Biswal, 2013. Effect of Withania somnifera (Ashwagandha) on the development of chemotherapy-induced fatigue and quality of life in breast cancer patients.
- Kaul, 2017. Ashwagandha for Cancer Metastasis: Bioactives and Basics of Their Function.
- Dutta, 2019. Withania Somnifera (Ashwagandha) and Withaferin A: Potential in Integrative Oncology.
Be careful about
- do not mix with sedatives (Triazolam)
- be careful if you have low blood pressure
- may not be suitable for people with Hyperthyroidism
- do not use when pregnant
- can skew blood test results of thyroid hormones and digoxin
Products
iHerb Now Foods 90 capsules 450mg, min. 2.5% Total Withanolides
Swanson 60 caps 250mg KSM-66 extract (it should have at least 5% withanolides).
In powder (as it is easy to mix in water). But withanolides amount is not guaranteed. Powder dosage from Bulk Supplements would be about 1-2 grams a day.
Melatonin
Melatonin has synergy with vitamin D3, berberine, ALA and pterostilbene. I consider melatonin as one of the TOP 10 most promising supplements in complementary cancer treatment.
- Wang, 2012. The efficacy and safety of melatonin in concurrent chemotherapy or radiotherapy for solid tumors: a meta-analysis of randomized controlled trials.
- Lang, 2012. Benefits of Melatonin in Solid Tumors When Used Concurrently With Chemotherapy
- Seely, 2012. Melatonin as adjuvant cancer care with and without chemotherapy: a systematic review and meta-analysis of randomized trials.
- Xin, 2015. Melatonin as a treatment for gastrointestinal cancer: a review.
- Showing anti-metastatic potential (Borin, 2015; Hill, 2015)
- May slow down the tumour growth (Paroni, 2014.; Zuccari, 2015)
- May increase radiotherapy effectiveness (Mihandoost, 2014; Alonso-Gonzáles, 2015)
- Reduces uptake of glucose (Hevia, 2015)
- Posadszki, 2018. Melatonin and health: an umbrella review of health outcomes and biological mechanisms of action
- Lissoni, 2018. Five Year-Survival with High-Dose Melatonin and Other Pineal Hormones in Advanced Cancer Eligible for the Only Palliative Therapy
- Wang, 2018. Therapeutic strategies of melatonin in cancer patients: a systematic review and meta-analysis
Be careful about
- don’t overdose melatonin, the daily dose should be probably under 50mg (though I know some people are taking more). The protocol is using 30mg as a daily dose which I believe is on both safe and efficacy side.
- Interactions with medication see this article
Important point
Do not take melatonin in the morning! It is closely linked to circadian rhythm of the body and it may be pro-cancer when taken in the morning.
“Melatonin injections given in the morning have been found to stimulate cancer growth while injections in the evening contribute to tumor regression.” (Bartsch, 1981; Blask, 1991)
Consider
- To use as pre-treatment before radiotherapy (Najafi, 2017; Farhood, 2019). To be taken about 30 to 60 minutes before the treatment, as it has the peak blood levels between 30 to 100 minutes. Consider also adding quercetin and curcumin.
- Be aware of article “Should Supplemental Antioxidant Administration Be Avoided During Chemotherapy and Radiation Therapy?” by Lawenda, 2008 before you take this decision. Consider, that study Berk, 2007 mentioned in Lawenda doesn’t make much sense, as there was many hours delay between taking melatonin and radiation therapy. Melatonin blood levels decrease considerably after 3 hours.
More information
Products
Any product which has 10mg in a pill.
PINK zone – Pyrcon
Pyrcon (Pyrvinium; pyrvinii embonas)
Important against cancer stem cells.
Comprehensive, thorough article on CancerTreatmentsResearch site. I will keep my post here short as all information are there.
Dosage to be reviewed yet. I would preliminary suggest to take it once in a month.
Be careful about
- Pyrcon colours your stool in red color, even after a couple of days (don’t get spooked by it)
Magnesium
Best add food high in magnesium. If you want to supplement, do occasionally, not daily. Best probably a magnesium citrate. Magnesium will support effects of vitamin K2 and vitamin D3.
What we may consider to add to the protocol – candidates?
For specific cancers
Loratadine (or Desloratadine). Olsson, 2018. Effects of antihistamine use on survival in breast cancer. Alternatively cetirizine (Zyrtec).
Beta carotene. Related to re-activation of HOXA5 (wiki) tumor suppressor.
Teo, 2016 (Medical Express article) Lab cell study shows that HOXA5 protein acts as tumor suppressor in breast cancer
Treating colon cancer with vitamin A
Retinoic acid and HOXA5 Yang, 2013
Retinoic acid (RA) wiki. RA is a metabolite from enzymatic conversion of beta carotene.
Flamini, 2014. Retinoic acid reduces migration of human breast cancer cells: role of retinoic acid receptor beta.
ScienceDaily article Can vitamin A turn back the clock on breast cancer?
Huelsken, 2015 HOXA5 Counteracts Stem Cell Traits by Inhibiting Wnt Signaling in Colorectal Cancer * Induction of HOXA5 eliminates cancer stem cells and prevents metastasis
Fucoidan. Promising results in double blind randomised clinical study (Tsai, 2017) in patients with metastatic colorectal cancer. Patients with standard treatment + fucoidan had disease control rate DCR 92,8%. Patients with only standard treatment had DCR 69,2%. DCR is defined as the percentage of patients with advanced or metastatic cancer who have achieved complete response, partial response and stable disease. Standard treatment was FOLFIRI+bevacizumab.
Maybe
Vitamin C orally. I would think it is a good idea that you can dilute let’s say 500mg of C in water and use for swallowing the pills. The reason is that vitamin C is showing strong synergy with Alpha Lipoic Acid, vitamin K2, quercetin, curcumin and doxycycline.
Reishi. Extract standardised to 30%+ of polysacharides; or extract focused on triterpenes (the first has more wide spectrum effects on health, while the latter is more cancer-focused). Reishi can give you a huge boost after chemotherapy and can help you to recover. It is also very good for liver health, better sleep and supports anti-cancer immunity.
Pre-treatment might help to sensitise some cancers to the treatment (lapatinib Cubano, 2014; erlotinib Suárez-Arroyo, 2014). It is one of those supplements which is usually possible to take also during chemotherapy, as it has low potential of interactions.
Shiitake (Lentinus edodes). Good combo with reishi. Probably two of the best medicinal mushrooms you can possibly use in cancers. Advantage is that it can be used also during standard treatment. Again, when buying, go for the standardised extract.
Sulphoraphane. I have been thinking for long time if to add it or not, but for now, I have decided not to. But you can add broccolli sprouts to your weekly diet regime. It is easy to grow them on your own as well.
A TIP, if you intend to buy a Sulphoraphane extract, don’t forget that body can make use of it only when it has a myrosinase enzyme. And there is only 1 product on the market with myrosinase (as far as I’m aware) which is Broccomax from Jarrow.
Remember, do not add sulphoraphane during main oncological treatment (kill phase) because it activates Nrf2 which may decrease effects of the treatment.
Genistein. The genistein is one of the supplements, which have high coverage regarding metabolic effects on cancers.
Zinc. You can supplement occasionally. Zinc is good for immunity and more (Fong, 2010) and also can reduce excess of copper. Zinc picolinate form seems to be ok.
Selenium. Supplement occasionally. Avoid in prostate cancer (Kristal, 2013; link; link). It benefits immunity as it points it more towards Th1 type (Hoffmann; 2010). Make sure you buy organic form of selenium, like selenomethionin. As anorganic forms are harmful! Chen, 2013.
Important point
Be careful to avoid anorganic forms of selenium! See from Chen, 2013:
“Inorganic Se, sodium selenite, only provided short-term inhibition of primary tumor growth, failed to reduce and possibly exacerbated metastasis.”
Cimetidine (Tagamet). It seems interesting. First, it helps bioavailability of mebendazole. Second, it may have further anti-cancer effects on its own Pantziarka, 2014; Dana, 2017; Jameson, 2015 (phase II trial), but compare with Jameson, 2018.
Syrosingopine. Blocking lactic acid transport out of the cancer cells. Synergical with merformin and diclofenac.
Probiotics
- Doxycycline negatively affects microflora of the gastrointestinal tract. I suggest to supplement probiotics after doxy, during the mebendazole month.
- Use probiotics with inulin, not with FOS!
Both FOS (Fructooligosaccharides) and inulin are prebiotics = they serve as food for probiotics. But when bifidobacterias ferment FOS, result is mainly acetate and lactate. While when they do ferment inulin, result is mainly butyric acid (butyrate; Rossi, 2005). It is important nuance to increase benefits and avoid risks (role of acetate and lactate will be discussed later in this article). - Sivan, 2015. Commensal Bifidobacterium promotes antitumor immunity and facilitates anti–PD-L1 efficacy.
- IFL Science article. Just One Antibiotic Treatment Can Alter Your Gut Microbiome For A Year.
- Liver cancer (Li, 2016. Bifidobacterium). Colon cancer (Lee, 2008 Bifidobacterium adolescentis). Yin, 2011 Bifidobacterium longum.
- Breast cancer. Lactobacillus acidophilus (Maroof, 2012). L. helveticus (Perdigón, 2005)
- Anti-cancer immunity. Choi, 2006 L. acidophilus and L. casei
- During irinotecan chemotherapy Mego, 2015
Inulin may have anticancer effects on its own. See article from 2020: “Prebiotics Boost Antitumor Immunity and Help Mice Fight Melanoma”
No
Low dose aspirin (article). I’m not sure about this one, because of the risk of bleeding. Especially, when we consider we can’t predict how it will be affected by all those other supplements. I mean, the risk is fairly low if you take just the low dose aspirin, but it is different when you take over 20 other supplements/drugs. Under these circumstances, my risk/benefit analysis goes against it. But I need to review this.
At ChristBeatCancer, Chris recommends to use a spoon of cumin instead.
Vitamin C intravenously. I would recommend to avoid and consider it a waste of money, as unfortunatelly, it has become business more than anything else. And all clinical studies I’m aware of failed to show any real results (Casciari, 2005; Stephenson, 2013; Welsh, 2013; Carr, 2014; Ma, 2014; Vollbratch, 2011).
Real I mean really real, like worth the money as IV C is very expensive (at least compared to the costs of supplements and drugs recommended in this protocol).
If you want to limit toxicity, there are many other supplements in this protocol working the same way or better, but much cheaper. If you want to improve fatigue, just buy some quality Reishi.
I don’t see any recent studies proving its anti-cancer effects in kill phase (when used in mega doses, where vitamin C is acting as an pro-oxidant). See e.g. Klimant, 2018; Carr, 2018. Nauman, 2018 systematic review do mention one study (Chapman, 2014) with PFS (progression free survival) increase in ascorbate group. The only one study I am able to find. But it had only 22 patients finishing the study, it cannot be taken seriously. You cannot use a statistical significance really on such a small sample. Where is this hype about Vitamin C IV coming from then? See below

If you by any reason really fancy your intravenous vitamin C (and don’t believe me or studies), make sure you pre-treat your body with mega dosage of lycopene, as it gives your C a giant boost (Riso, 2004). Alternative is a dish containing cooked tomatoes (lycopene in tomatoes increases by cooking). Another rich source of lycopene is a water melon.
There are so many proponents of vitamin C IV, but I have not seen anyone recommending this absolute must synergy with lycopene.
B vitamins. I am not sure about effects of some of B vitamins on some of the cancers. As it doesn’t offer considerable benefits, there is no point of having to risk anything. This is the case also for Niacin (B3) which I used to consider the best choice from B vitamins in cancers see Piacente, 2017. Nicotinic acid: A case for a vitamin that moonlights for cancer?
There might be one exception with B12, which might be needed because of metformin use (Alharbi, 2018). But I would not supplement this without been diagnosed with deficiency, as the risk of it is quite low and involves long term use + high dosages: “Individuals with T2DM treated with metformin, particularly those who use metformin at large dosages (> 2,000 mg/day) and for a longer duration (> 4 years), should be regularly screened for vitamin B12 deficiency and metformin is associated with B12 deficiency”.
I would agree with this recommendation: “Just have your levels checked every year if you take metformin, for patients with levels over 300 mg/mL, taking a supplement isn’t necessary.” (link).
NAC (N-acetylcysteine)
-
- Protects kidneys (Moussa, 2013). This is very important, as so many supplements and drugs will be demanding to kidneys.
- May improve EGCG (Lambert, 2008)
- Monti, 2017. Pilot study demonstrating metabolic and anti-proliferative effects of in vivo anti-oxidant supplementation with N-Acetylcysteine in Breast Cancer.
MCT-4 “Patients taking high dosages of NAC saw their levels of the ‘transporter’ protein fall by more than 80%, drastically reducing the ability of the cancer cells to feed off neighbouring cells.” - There are some worries though.
N-Acetyl Cysteine: A Warning Shot. Lowe, 2019.
And Breau, 2019. Shyam, 2018. Due to this uncertainty, I prefer not to add it, though we may re-evaluate later.
Fish Oil (DHA, EPA)
- I would suggest to avoid because of immunosuppressive effects (link). E.g. decreasing CD4+ lymphocytes.
Avoid at all costs
Cesium Chloride (dangerous quackery). Only for business and risk of death by hypokalemia.
Jim Kelmun Protocol (maple syrup, baking soda). The baking soda may work only if injected locally into the tumour. Otherwise, taken orally, it is a nonsense quackery.
Gerson Protocol. Only business offered by clinics for money, no real effect on cancers. Only very expensive marketing fairy-tales (2 weeks at Gerson clinic in Hungary is 6900 euro; recommended lenght of stay can be even over 12 months). The dietary recommendations are ok though like juicing (celery, ginger, broccoli, carrots etc). B12, pancreatic enzymes, thyroid hormones are doubtful. Not sure about supplementing iodine (would need to look deeper into it). The main controversy of this method is that it is presenting itself as a cure, which it can never be and that it costs fortune.
Coffee enemas. The role of glutathion S-transferase (GST) is unclear whether it is beneficial or harmful. Cafestol and Kahweol have some anti cancer effects in studies in vitro. But you can get those by drinking coffee as well. Gerson forbids coffee, though the coffee is beneficial for general public and in cancers as well see e.g. metastudy Yu, 2011 “increase in consumption of 1 cup of coffee per day was associated with a 3% reduced risk of cancers”.
Budwig Protocol. Very difficult to follow up properly. Especially to find out correct flax variety (if you are unlucky and pick wrong one in Omega3-Omega6 ratio, you will actually do the opposite of what Budwig intended you to do). Also it doesn’t make sense to eat quark (cottage cheese) as it has cystein (which is beneficial), but also methionin (which is most probably harmful). And Budwig used quark only to support bioavailability of flax seeds, as those sulphur-based amino acids do help water solubility of fatty acids from flax. So all in all, this protocol is currently out dated. Also I don’t see much potential of this protocol to help our metabolic blockade strategy.
B17 Amygdalin (Laetrile; B-17). It is a compound extracted from peach stones. Until further evidence, we should consider this only as a money making scam from Mexico, which has spread elsewhere. So far, it works to some extent only in in vitro studies (like hundreds of other substances). I knew a few people from Czech Republic who bought it from Mexico, but it did not help them at all (it only costs them a lot of money). One of them was my friend who used IV B-17 for a long time and had progression on it.
Statistics from clinics in Mexico are pure fabrications. This particular drug is very polarising in internet discussions, compared to others. I would credit it to paid propaganda by the clinics and many anecdotes are also written by people who are part of its distribution chain = they benefit from it. There might be some people, to whom it did help in some way (some true testimonies), but they are rare. Majority of people using only B-17 would be dead – dead cannot testify. In a certain natural treatment cancer group on FB, when I wrote my opinion on B-17, I was attacked harshly, accussed of being paid by big pharma and being a troll. Attacked by those, who scam people by spreading lies and robbing them of their money.
Calcium. Do not supplement any calcium why on this protocol. There are regular dose of vitamin D3 which will increase calcium absorption from food. There is no need to extra calcium.
Multivitamins / multiminerals. Do not supplement any of those. Focus on your heatlhy diet. Avoid especially vitamin E (tocopherols) which would inhibit anticancer effects of tocotrienols.
Copper. Copper is promoting cancer development. Avoid supplementing any product with copper and try to limit food high in copper. There is no need to fuel the growth. The only exception where copper is to be supplemented is when you opt to try Antabus (disulfiram) as anti-cancer drug, as it needs copper to make disulfiram/copper compounds.
Alcohol. Avoid as it converts to acetate. It also suppresses Th1 immunity response, which is beneficial in cancers (Latif, 2002, link; Waltenbaugh, 1998, link; Svistunov, 2012, link; Liu, 2011, link).
What blood values to monitor during the protocol?
Two most important are liver and kidney values.
- Liver health including:
P_AST (under 0,75)
P_ALT (under 0,78)
P_GGT (under 0,72)
P_ALP (under 2,2)
Bilirubin (under 20 μmol/l)
- Kidney health (creatinine, UREA, urea acid, eGFRepi)
You should also monitor
- Glucose (important, as there are more supplements which have direct effect on glucose like metformin, berberine, HCA and few others). Also curcumin may increase the effects of other blood sugar medications.
- Cholesterol values including:
Total cholesterol
LDL (low-density lipoprotein cholesterol, also called “bad” cholesterol)
HDL (high-density lipoprotein cholesterol, also called “good” cholesterol)
Triglycerides
- Iron levels (occasional supplementation might be useful, as EGCG, ALA and curcumin can diminish the levels). But do supplement only when you are in deficit based on blood tests. As otherwise, in general supplementing iron is not good idea in cancers, similar to the copper. This is here just to warn about the theoretical risk of anemia for your to be aware.
- 25-hydroxyvitamin D blood level. You should balance between 50 to 100 ng/mL. You should definitely go around 50, but watch to keep it under 100. Careful with results evaluation, sometimes the result can be in nmol/liter, not in ng/mL. Use converter to get ng/mL value.
- Blood pressure. Many of the supplements have possibly pressure lowering effect. If you normally do have low pressure, be careful and check your blood pressure on regular basis. Very low blood pressure may cause diziness, even fainting (short loss of consciousness).
Then there are some values, which may indicate how you are doing related to cancer treatment:
- CRP (in general, the lower, the better)
- Lactate dehydrogenase (LDH) (in general, the lower, the better)
- AGR (Albumin to Globulin Ratio) – in general, the higher, the better
- Albumin (in general, the higher, the better)
And there are also
- cancer specific markers
which I won’t be discussing here, as they are very individual, based on what cancer patient has and the topic is very complex.
Possible targets of individual substances in the protocol
I want to repeat something essential: this protocol aims to simultaneously target key metabolic pathways used by cancer cells for growth and survival. Blocking one metabolic pathway (i.e. glucose metabolism) at a time is not effective, as cancers are able to use other energy sources for their survival. It is like to be on a 4-way crossroad, with you blocking one way and thinking the cars cannot move any more.
We are planning to block metabolism in 3 major areas which are related to
- Glucose
- Glutamine
- Fatty Acids
I will link thorough visualisation of this approach, as presented by Jane McLelland in her book (you can purchase directly on her webpage) How to Starve Cancer.
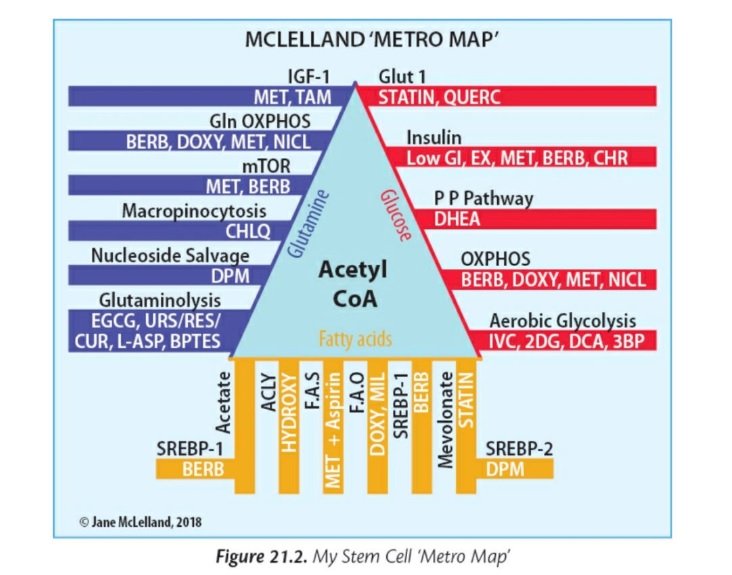
ORANGE zone – Fatty Acids Metabolism
Very important role of acetate. When glucose metabolism is being blocked, the more and more attention of cancer cells goes to glutamine and acetate.
What is acetate? Acetate is a precursor of acetyl-CoA, which is used by cells for the synthesis of fatty acids and cholesterol to build up the cell membrane.
Therefore acetate is used by tumour cells as an important bioenergetic fuel or as a nutritional source to support lipid biosynthesis.
- Tumors with high ACSS2 (Acetyl-CoA synthetase 2) expression are acetate avid (have hunger for)
- ACSS2 is highly upregulated in multiple cancer types
- A large increase in circulating acetate levels may benefit some types of cancer (for example, breast, ovarian and lung cancer)
- [11C]acetate has demonstrated excellent potential as an alternative positron emission tomography imaging probe for cancer. More studies on why some but not other tumours are [11C]acetate avid, and correlating these data with the expression of acetyl-CoA synthetases will aid in deciphering the exact manner by which acetate metabolism supports tumour growth and help in stratifying patients for future anti-ACSS2 therapy (Schug, 2016).
More info
- Hossios, 2014. Acetate metabolism in cancer cells
- Kamphorst, blog, 2014. Acetate helps hypoxic cancer cells get fat
- Schug, 2015. Acetyl-CoA Synthetase 2 Promotes Acetate
Utilization and Maintains Cancer Cell Growth
under Metabolic Stress - Korri, 1985. Avoid alcohol as it converts to acetate
- CancerTreatmentsResearch article
- Bose, 2019. Acetate Metabolism in Physiology, Cancer, and Beyond
Tips for tailoring
- Cisplatin resistance in bladder cancer (Kim, 2019). Think about adding Orange Zone supplements, especially SREBP2 inhibitors, during the chemotherapy.
FAS inhibitors (fatty acid synthase)
FAS is a major enzyme required for the conversion of dietary carbohydrates to fatty acids.
The expression level (its up-regulation) of FAS is related to cancer progression, aggressiveness and metastasis
- EGCG (Pan, 2007)
- luteolin
- quercetin (Sultan, 2017)
- fisetin
- metformin (Cantoria, 2014)
- dihydrocurcumin
Over the counter drugs
- Cerulenin is other possible option for an existing drug which can be repurposed as FAS inhibitor in cancers.
- Orlistat – weight loss drug.
Be careful about
- Do not confuse FAS as Fatty Acid Synthase with Fas as Fas cell surface death receptor (also known as APO-1 or CD95) (Buckley, 2015)
Fatty Acids Oxidation (FAO)
- doxycycline (De Francesco, 2017) with combination with Vitamin C
Cells generate energy by breaking down Fatty Acids via oxidation (FAO). So we can presume we should inhibit FAO.
Ma, 2018 “FAO is activated when the environmental glucose becomes limited. On the other hand, inhibition of FAO switches energy metabolism from fatty acid to glucose oxidation.”
Note “glycolysis and FAO occur simultaneously in cancers” as function of FAO cannot be fully replaced. That is a reason why blocking both is beneficial even at the stage where glucose metabolism is the main factory for the fuel.
Tips for tailoring
- focus on FAO in prostate cancer (Koundouros, 2019; Watt, 2019)
- BRAF mutated melanoma (Aloia, 2019) ” The upfront and concomitant inhibition of FAO, glycolysis, and MAPK synergistically inhibits tumor cell growth in vitro and in vivo.”
- FAO may be of major importance to limit metastasis: “Among metabolic pathways, FAO is the most energy-efficient way to generate ATPs to satisfy the energy needs of cancer cells and is perhaps particularly crucial for disseminated tumor cells, which must withstand the selective pressure of metastatic colonization.” (Chen, 2019).
See also Park, 2019: “We found that tumor cells undergo dramatic metabolic reprogramming towards fatty acid oxidation (FAO) for successful lymph node metastasis.”
Confusion point
- Aiderus, 2018 comes to this conclusion: “Our findings suggest that FAO is downregulated in multiple tumour types, and activation of this pathway may lower cancer cell proliferation, and is associated with improved outcomes in some cancers.” Can someone explain the result of this in vitro study in relation to all other studies?
Compare with Wang, 2018.
Inhibition of ATP citrate lyase / ACLY inhibitors
ACLY is a strategic enzyme linking both the glycolytic and lipidic metabolism. The enzyme has other roles, including cholesterol biosynthesis, so inhibitors against this enzyme could also be useful toward controlling cholesterol levels.
- HCA Hydroxycitric acid (Garcinia Cambogia)
HCA has been discussed in more depth in METABLOC section.

Picture Source
Tips for tailoring
- super charge in liver cancer (Pope, 2019; survival analysis)
- colon cancer (Wen, 2019)
- cervical cancer (survival analysis)
- acute myeloid leukemia (Wang, 2019; Low expression of ACLY associates with favorable prognosis in acute myeloid leukemia)
SREBP2 inhibitors – targeting ACSS2
When ACLY is inhibited, tumor cells will – as workaround – express ACSS2 enzyme to convert acetate to acetyl-CoA (source).
ACSS2 level is modulated by SREBP2 (Heidegger, 2018) which can be decreased by:
- apigenin (Wong, 2015)
- luteolin (Wong, 2015)
- metformin (Zhang, 2018)
- dipyridamol (Pandyra, 2014). Targeting tumor cell metabolism via the mevalonate pathway: Two hits are better than one. “Dipyridamole strongly synergized with and potentiated the pro-apoptotic effects of atorvastatin”
More info:
- Wong, 2017 Apigenin and luteolin display differential hypocholesterolemic mechanisms in mice fed a high-fat diet.
“These results revealed that apigenin suppressed the biosynthesis of cholesterol, whereas luteolin promoted the elimination of cholesterol.“ - Wen, 2018 Downregulation of SREBP inhibits tumor growth and initiation by altering cellular metabolism in colon cancer

Tips for tailoring
- ovarian cancer during cisplatin chemo (Zheng, 2018)
SCAP/SREBP-1 inhibition
Inhibition of the activity of SREBP-1 decreasing the synthesis and accommodation of fat and impeding the glucose uptake.
RED zone – Glucose Metabolism
Warburg effect refers to the observation that even in aerobic conditions (when free oxygen is easily available), cancer cells tend to favor metabolism via glycolysis rather than the much more efficient oxidative phosphorylation pathway (OXPHOS). Which is strange indeed, because OXPHOS will produce as much as 15 times more ATP then glycolysis, from the same start investment. ATP is the final product, and you can think of it as money for which you can pay for a lot of services in the body.
Glycolysis is used by all cells in the body for energy generation. In normal cells, the final product of glycolysis is pyruvate in aerobic settings (with oxygen) and lactate in anaerobic (with lack of oxygen) conditions.
Tumor cells do differ. Even if they do have oxygen, and they do aerobic glycolysis, they are not satisfied with last product to be pyruvate, they convert it into lactate. Somehow, tumor cells fancy lactate and this must have a reason..
Therefore at the RED zone, we are trying to block every step of this process. Starting with glycolysis (process of breaking down glucose) up to setting obstacles for cancer cells when they are utilising the lactate.
Recap
- Tumor cells are producing large volumes of lactate
- As a consequence of such amounts of lactate there is an acidification of the extracellular pH in tumor microenvironment. Meaning, they are making their neighborhood sort of lactaty (acidic).
- For lactate role in cancers review, scroll back to VIOLET zone – Laurent Schwartz METABLOC protocol.
Note, if you understand above, you can see how silly are internet quacks who advocate eating alkaline food to combat cancer. The acidification is not caused by food in any sense. And you can not tackle it by drinking soda bicarbona with maple syrup neither. The only chance to handle it is to target this part of metabolism directly within the cancer cells.
Be careful about
- Do not forget to check your cancer and its relation to fructose. Santhekadur, 2019. The dark face of fructose as a tumor promoter
- Avoid fructose for example in pancreatic cancer (link; link) and small intestinal cancers (Port, 2012)
- Tumor Growth Fueled Directly by High-Fructose Corn Syrup. Article. Corn syrup can be added everywhere, read the labels.
Blocking glycolysis (Liu, 2016)
- METABLOC (ALA + HCA)
- EGCG
- pterostilbene
- quercetin
- curcumin (Melnick, 2015)
Targeting GLUTs
GLUTs are enzymes transporting glucose. Small transport cars which are driving loads of glucose in and out of a cell. Cancers are big customers buying these transport services. Their goal is to have as much GLUTs as possible working for them.
- Tumor cells exhibit elevated levels of glucose uptake, a phenomenon that has been capitalized upon for the prognostic and diagnostic imaging of a wide range of cancers using radio-labeled glucose analogs (PET Scans).
Anti-cancer attempts are trying to regulate amount of GLUTs, or limit their carry capacity, or load them with passengers similar to glucose (heroes in disguise). Or spam GLUTs with compounds which are competing for GLUTs services with glucose (I’m sorry Ms. Glucose, the bus is full already with Mr. Melatonin. Next coming in two hours, ma’m).
GLUT-1
There are many studies correlating GLUT-1 expression with overall survival and poor prognosis. In simplicity, the more GLUT-1 expression, the shorter survival (Komaki, 2019; Kim, 2019; Haber, 1998; Tanaka, 2011). It may not apply to all cancers.
Yu, 2017. The prognostic value of GLUT1 in cancers: a systematic review and meta-analysis. Increased expression of GLUT1 was associated with:
- unfavorable overall survival
- poorer disease-free survival
- poor differentiated tumors
- positive lymph node metastasis
- larger tumor size
Enough reasons to really focus on GLUT-1.
- apigenin
- melatonin (Granchi, 2016)
- curcumin (Gunnink, 2016)
- quercetin (Hamilton, 2016) inhibits glucose transport by binding to an exofacial site on GLUT1
- atorvastatin (Malenda, 2012) “statins can effectively inhibit glucose uptake by tumor cells”; Note that atorvastatin can skew the result of PET scan (with 18F-FDG PET).
- resveratrol (Zambrano, 2019)
- genistein (direct competitive inhibitory effect on GLUT 1)
- HDAC inhibitors (will be mentioned later) can down-regulate GLUT-1 (Wardell, 2009)
- EGCG (Wei, 2018; Ojelabi, 2018)
Be careful about
- Cok, 2011. Berberine acutely activates the glucose transport activity of GLUT1. Fortunatelly, the effect seems to be acute, starting after 5 mins and peaking at 30 min mark. Can be this effect reverted by other supplements? E.g. here Zhou, 2007 by genistein.
GLUT-4
Glucose Metabolism blockade
- berberine (Mao, 2018)
- melatonin (Hevia, 2015. Melatonin uptake through glucose transporters: a new target for melatonin inhibition of cancer )
HIF-1 inhibition
Hypoxia is frequently observed in solid tumors and also one of the major obstacles for effective cancer therapies. Cancer cells take advantage of their ability to adapt to hypoxia. Hypoxia-inducible factors (HIFs) are the key factors that help them to achieve this.
The hypoxia-inducible factor 1 (HIF-1) pathway enables tumor cells to survive by changing glucose metabolism toward a glycolytic phenotype.
HIF-1 may up regulate the glucose transporters (GLUTs) and the increase in production serves as adaptation of cancer cells to the hypoxic environment.
Non-protocol substances
- Chrysin. But doesn’t work because of very low bioavailability.
EZH2
A gene suppresor. When it becomes overexpressed, many tumor suppressor genes that are normally turned on, are turned off.
“The correlation between HIF-1 and EZH2 is an interesting but yet uncharted aspect of tumor biology. There are few scientific studies connecting hypoxia, HIF-1, and EZH2 during tumor formation or tumor progression. The majority of such studies concord with the idea that hypoxia in general and HIF-1 in particular increase EZH2 expression.” (Papale, 2018).
The overexpression of EZH2 has been correlated with many cancers, such as prostate, breast, bladder, whereas other kinds of cancer, such as B-cell lymphomas or other forms of breast cancer, can be promoted by specific mutations (Tan, 2014).
Keep in mind that EZH2 inhibitors are useless or even harmful in those cancers characterized by a loss of function of EZH2. “Even harmful” would need to be checked, but it is a tip for tailoring, if you find your cancer is overexpressing EZH2, you can focus on this One-Two blow (HIF and EZH2).
- Sahebkar, 2017. Naturally occurring anti-cancer agents targeting EZH2
MCT1 inhibitors / transporting lactic acid INTO
blocking acetate and lactate take up to cancer cells
- Luteolin
- Quercetin
- Silybin
- Atorvastatin (inhibits the efflux (spitting out) transport of L-lactic acid; this inhibition may cause an accumulation of intracellular L-lactic acid; Leung, 2017)
- Diclofenac
MCT4 inhibitors / transporting lactic acid OUTSIDE
More info on MCT1 and MCT4
- Long, 2018 Downregulation of MCT4 for lactate exchange promotes the cytotoxicity of NK cells in breast carcinoma
- Black, 2018 Selective inhibition of the lactate transporter MCT4 reduces growth of invasive bladder cancer
- Benjamin, 2018 Dual Inhibition of the Lactate Transporters MCT1 and MCT4 Is Synthetic Lethal with Metformin due to NAD+ Depletion in Cancer Cells *this study has documented synergy between atorvastatin and metformin
Note, Syrosingopine may have extreme synergy with Metformin.
Article Lethal combination: Drug cocktail turns off the juice to cancer cells
Can we make cancer cells suffocate with their own lactate?
PKM2 inhibitors (glycolytic enzyme pyruvate kinase M2)
Cells that express PKM2 produce more lactate and consume less oxygen.
- Metformin (Su, 2019)
There are two other related targets linked to PKM2, these are HK2 (hexokinase 2) and PFKFB3 (6-phosphofructo-2-kinase/fructose-2,6-biphosphatase 3).
Imagine 3 things: a kitchen sink, a sink plug and a water tap.
Cancers want as much water through the tap as possible, and as less water as possible to be drained out through the sink hole.
The more HK2 and PFKFB3, the more water goes through the tap (like it would widen the pipe). The more PKM2, the bigger the plug is, keeping more water for the cancer in the sink. PKM2 is the plug.
So we want to reduce HK2/PFKFB3 to close the tap (narrow the pipe) and also we want to reduce PKM2, to unplug the sink and let the water run out.
During glucose starvation
- Pyrvinium (Esumi, 2004)
OXPHOS (oxidative phosphorylation)
Target in some cancers. Especially ovarian cancer (Nayak, 2018).
- metformin
- berberine
LDH-A inhibitors (lactate dehydrogenase)
Inhibiting LDH-A and LDH-B can help blocking lactate exchange between tumor and stroma (Mishra, 2019). Decreasing LDH-A will block it in cancer cells and LDH-B in stromal cells (as we talked about treacherous CAFs). “CAFs are offering available glucose to cancer cells and utilizing lactate secreted by their masters.”
Lactate dehydrogenase is an important predictive factor in cancers. The lower is serum value, the better is treatment outcome. The LDH levels might be linked to metastasis potential as well.
Liu, 2019. Prognostic significance of serum lactate dehydrogenase in patients with breast cancer: a meta-analysis.
Long, 2019. Pre-treatment Serum Lactate Dehydrogenase Predicts Distant Metastasis and Poor Survival in Nasopharyngeal Carcinoma.
Pelizzari, 2019 in metastatic breast cancers. Wei, 2018 in colorectal cancer. Mori, 2019 in prostate cancer. There are many other recent studies, check Google Scholar database.
More info
- CancerTreatmentsResearch article. Glucose Absorption Inhibitors to Inhibit Tumor Growth.
BLUE zone – Glutamine Metabolism
As a tumor grows, it rapidly outgrows its blood supply, leaving portions of the tumor with regions where the oxygen concentration is significantly lower than in healthy tissues. It is called tumor hypoxia.
Glutamin is becoming an important source of energy for cancers, especially under such hypoxic conditions (Corbet, 2016).
Note that in case of total blockage of glutamine metabolism, cancers would opt for asparagine (Zhang, 2014).
Cells can overcome glutamine deficiency through the use of asparagine for proliferation and protein synthesis.
You can counter-act this by opting for a low-asparagine diet. Foods rich in asparagine include dairy, whey, beef, poultry, eggs, fish, seafood, asparagus, potatoes, legumes, nuts, seeds, soy and whole grains (article).
I would say, the later the stage, the higher probability the metabolism will shift “the glucose to glutamine” ratio more towards the latter.
There is no way to know what your cancer prefers at a current moment. Maybe you can get some picture if you would monitor your cancer regularly by both PET scans (with a glucose attached with a radioactive component – called 18F-FDG) and Glutamine PET scans. But the latter is still nonstandard in oncological care and is done rarely.
This is another reason why we really need to block all pathways, otherwise we would be just guessing in the dark and if we guess, our guess can be wrong.
- Wappler, 2020. Glutamine deprivation counteracts hypoxia-induced chemoresistance
- “Autophagy inhibition by chloroquine significantly enhanced glutamine starvation induced growth inhibition and apoptosis activation. Asparagine deprivation by L-asparaginase exacerbated growth inhibition induced by glutamine starvation and autophagy blockage. Similar to glutamine starvation, inhibition of glutamine metabolism with a chemical inhibitor currently under clinical evaluation was synthetically lethal with chloroquine and L-asparaginase, drugs approved for the treatment of malaria and leukemia, respectively.” Li, 2017
Tips for tailoring
- Ovarian cancers. Focus on Glutamin and Fatty Acids. And there will be different targets for poorly and highly aggresive types (article)
Blocking glutaminolysis
Matés, 2020. Therapeutic targeting of glutaminolysis as an essential strategy to combat cancer
- EGCG (glutamate dehydrogenase inhibitor GDH; substance that targets the conversion of glutamate to α‐KG)
- metformin (Fendt, 2013; Kim, 2018) works with synergy with glutaminolysis blockade
- Curcumin + Resveratrol + Ursolic acid combo. Lodi, 2017.
Other possible targets in glutaminolysis are glutamine‐mimetic compounds and glutaminase (GLS) inhibitors (Zhang, 2017).
Check F‐FGln PET scans Dunphy, 2018
Inhibition of ASCT2 (glutamine transport)
Reduces growth and glutamine uptake by cancer cells; it is a major transporter for glutamine uptake; inhibition will reduce intracellular glutamine.
- resveratrol (pterostilbene) Liu, 2018
Other possible substance is retinoic acid (vitamin A) and cysteine (NAC; has also benefit in protection against kidney toxicity; is one of the substances on which Budwig protocol is based on).
Whiteman, 2017. Cancer cell growth halted with cold and flu drug
Targeting Cholesterol
For detailed info about this topic see article on CancerTreatmentsResearch website.
Some of the cancers may use cholesterol as an alternative fuel including:
– some of breast cancers (link)
– advanced prostate cancer (Peck, 2014): Tumors display distinct metabolic programs, and altered lipid metabolism is emerging as an important process in cancer.
– Yue, 2014 reports that aberrant cholesteryl ester accumulation is found in advanced prostate cancers with PTEN loss and PI3K/AKT activation. Importantly, inhibition of cholesterol esterification impaired cancer aggressiveness.
Cholesterol synthesis pathway inhibitors
- atorvastatin (Kuzu, 2016)
- tocotrienols (inhibiting HMG-CoA reductase / Mevalonate pathway)
Inhibit storage of cholesterol as lipid droplets (ACAT1 inhibitors)
- piperine
- honokiol
Inhibiting the growth of new blood vessels (Angiogenesis inhibitors)
Wang, 2015. Broad targeting of angiogenesis for cancer prevention and therapy
VEGF inhibition (slows down creating of new supply veins to tumours)
- AKBA boswellia serrata
- tocotrienols gamma/delta
- apigenin
- mebendazole
- silymarin
- curcumin
- fisetin
- quercetin (Song, 2017)
- honokiol
- piperine
- melatonin (Paroni, 2014; mouse study. Melatonin was able to significantly block growth of new veins; Zuccari, 2015)
Check TED “Can we eat to starve cancer?” about angiogenesis inhibitors.
VEGFR2 kinase inhibitors
- mebendazole (Bai, 2015)

http://mcr.aacrjournals.org/content/5/3/203

Telomerase inhibitors
Telomerase enzyme is responsible for unlimited dividing of the cancer cells. Each cell has a telomera, which is like a candle of life. Every lighting of this candle will make it a little shorter. Eventually, there will be no candle left. Cancer cells are cheating the death, by producing telomerase enzymes, they are enlarging the candle constantly. We want to block this option to cancers.
- curcumin
- melatonin + berberin (Deng, 2016)
- EGCG
- genistein
Evasion of anti-growth signaling
More info
- Amin, 2015. Evasion of anti-growth signaling: A key step in tumorigenesis and potential target for treatment and prophylaxis by natural compounds
p53 tumor suppresor re-activation
- pterostilben Schneider, 2010
- luteolin with EGCG Amin, 2010
- berberine Ortiz, 2014; Qi, 2014
- ginger extract Warin, 2014
- ashwagandha
- resveratrol Silva, 2014; Dumont, 2015
More info
- article Tumor-suppressor p53 regulates protein that stifles immune attack on cancer
PTEN activation
- honokiol (Liu, 2008)
- pterostilbene (Qian, 2018; Dhar, 2015)
- curcumin. Matsuda, 2012. PTEN activation helps anti-cancer effect of curcumin
Source of the picture link.
ARID1A activation
Important especially in ovarian, endometrial and uterine cancers (Wu, 2013). Increase dosage of pterostilbene/resveratrol in those. Also children neuroblastoma Sausen, 2013.
- resveratrol (indirectly through AKT inhibition)
Notch-1 inhibition
- ashwagandha
- curcumin
When tumor cells metastasize
More info
-
Jiang, 2015. Tissue invasion and metastasis: Molecular, biological and clinical perspectives
Anti-Metastatic Potential
PI3K inhibitors
- quercetin
- pterostilbene
- curcumin
Akt inhibition
Many cancers have hyper activated this pathway to grow faster and avoid cell death. Hyper active Akt helps metastasis and angiogenesis. It also helps to use more glucose (see Nitulescu, 2016).
- apigenin
- curcumin
- fisetin
- EGCG
- pterostilbene
Regulation of β-catenin activity
- curcumin
- quercetin
- silymarin
- Pyrcon (pyrvinium)
MMP-1
- fisetin
MMP-2
- mebendazole
- doxycycline
MMP-9
- AKBA
- curcumin
- EGCG
- pterostilbene
- quercetin
- doxycycline
Chronic inflammation
COX-2 inhibitors
- quercetin (Xiao, 2011)
- EGCG
- curcumin
- vitamin D3
- aspirin and ibuprofen (not added in the protocol, as explained in the previous chapter: What we may consider to add to the protocol – candidates?

Source of the picture link.
MIF inhibitors
- sulphoraphane (Tilg, 2015)
- EGCG (Park, 2012)
- curcumin
- loratadine (Claritin) or cetirizine (Zyrtec) Feily, 2013

Source of the picture link.
NF-κB inhibitors
- tocotrienols
- pterostilbene
- curcumin
- AKBA
- luteolin
- apigenin
Journey to immortality – make them mortals again
More info
- Mohammad, 2015. Broad targeting of resistance to apoptosis in cancer
Role of Bcl-2 family proteins in resistance to apoptosis
Inhibitors of Bcl-2 are
- EGCG
- curcumin
- gingerol
Hsp70, Hsp90
Proteins are over produced in cancers and protect cancer cells agains wide range of damage. Hsp70 serves to cancer cells like a batsuit to Batman.
- EGCG (Banerji, 2015)
ENOX-2 blockage
ENOX-2 has been discussed in details in EGCG chapter.
- EGCG
- capsaicin
Other targets
Effect against cancer stem cells (CSC)
The cancer stem-cell (CSC) hypothesis suggests that there is a small subset of cancer cells that are responsible for tumor initiation and growth, possessing properties such as indefinite self-renewal, slow replication, intrinsic resistance to chemotherapy and radiotherapy, and an ability to give rise to differentiated progeny (O’Flaherty, 2012).
Bighetti-Trevisan, 2019. Cancer Stem Cells: Powerful Targets to Improve Current Anticancer Therapeutics
- piperine (Rather, 2018)
- silymarin (Kumar, 2014; Raina, 2016)
- doxycycline with vitamin C (De Francesco, 2017; Scatena, 2018)
- Pyrcon (pyrvinium) Sahebkar, 2018 – inhibits mitochondrial function which is critical for the survival and growth of CSCs
Daniel mentions also Salinomycin on his web page, but it is not easily accessible (it might be used in veterinary medicine?) and it has high costs. So I guess it is not convenient to pursue.
Below scheme is suggested in De Francesco, 2019. In our protocol, the first hit is actioned by berberine and metformin. Second hit by doxycycline and berberine. And it is suggested to take doxycycline with vitamin C (orally).

Chemosensitizing and Reversal of Resistance Effect
- piperine (Li, 2018)
HDAC inhibition (Histone deacetylase)
- curcumin
- quercetin
- EGCG
- luteolin
- apigenin
- holy basil
Food with anti-HDAC activity Bassett, 2014. E.g. garlic (allicin), green tea (EGCG), cinnamon, ginger, basil, broccoli.
Mottamal, 2015. Histone Deacetylase Inhibitors in Clinical Studies as Templates for New Anticancer Agents
Source of the picture link
IGF-1R inhibitors
- apigenin
- curcumin
- EGCG
- pterostilbene
- quercetin
https://www.researchgate.net/figure/The-effects-of-IGF-1-and-IGF-1R-on-normal-and-cancerous-cells_fig2_309148630
5-LOX inhibitors
The 5-LOX pathway creates 5-HETE that helps to protect damaged cells from dying and leukotriene B4 a powerful inflammatory agent that may help cancer cells to spread.
- AKBA
- curcumin
- ginger extract
CXCR4 inhibitors
Important target to support during immunotherapy, especially using anti PD-L1 inhibitors (Tucker, 2020).
- AKBA (Zhao, 2015)
STAT3 inhibition
- Holy basil
- Curcumin
- AKBA
- Capsaicin
- Pterostilbene
mTOR inhibitors (Mammalian Target Of Rapamycin)
Important target in melanoma and breast cancers. High activity of mTOR leads to suppresion of autophagy.
We can fight it by suppresing mTOR by:
- EGCG (Srivastava, 2014)
- Curcumin
- Pterostilbene
- Apigenin (Tong, 2011)
- Quercetin
- Fisetin (Wang, 2018)
Or we can also support autophagy, by activators:
- Melatonin (Choi, 2013)
- Gamma Tocotrienol
- Magnolol
Wnt signaling pathway blockers
- EGCG
- curcumin
- quercetin
- Pyrcon (Zhang, 2014)
Inhibition of Sonic Hedgehog Signaling Pathway
PARP inhibitors
The PARP inhibitors act to stop the cancer cells DNA being repaired by PARP, so the damaged DNA stays at the critical level that causes cell to trigger its own death.
- quercetin
- fisetin
Tyrosine Kinase Inhibitors (TKI inhibitors)
- quercetin (Ferry, 1996)
- curcumin
TKI are often used in lung cancers, especially with some of the EGFR mutations. The most well known drugs are: 1st generation Gefitinib (Iressa), Erlotinib (Tarceva); 2nd generation Afatinib (Gilotrif); 3rd generation Osimertinib (Tagrisso). If you are going to use one of those, check for some synergies like Erlotinib + EGCG Milligan, 2009; Haque, 2015 or Afatinib + Withaferin A (withania somnifera extract) Chang, 2014.
ERK2 inhibitors (Otabe,2016)
Doing its work on MAPK pathway, often known as the RAS-RAF-MEK-ERK signal cascade.
Liu, 2018. Targeting ERK, an Achilles’ Heel of the MAPK pathway, in cancer therapy.
- luteolin
- quercetin
- fisetin
Aromatase inhibitors
Aromatase inhibitors work by blocking the enzyme aromatase, which turns the hormone androgen into small amounts of estrogen in the body. This means that less estrogen is available to stimulate the growth of hormone-receptor-positive breast cancer cells.
- melatonin (Mendendéz, 2018)
LACTB activators
- Kečkéšová, 2017. Check for breast cancers. γ-Bisabolene, one of the main components of Cardamom (and also in oregano, lemon and kubeb), is activating this tumor suppresing protein.
Inhibition of NADH-fumarate reductase system
Deprive mitochondrial energy production in tumour microenvironments.
- Pyrcon (pyrvinium) – pyrvinium localizes to mitochondria and induces apoptosis by inhibiting mitochondrial respiration (Xiang, 2015).
Myc inhibition
C-Myc regulation
May be important target in some brain cancers (Swartling, 2012).
PDK inhibitors
Blocking cancer cells possibility to make lactate from pyruvate. Discussed in more details in Metabloc chapter.
- alpha lipoic acid
Blockage of IL-6 (interleukin 6)
Both IL-6 and IL-8 blockage is important to limit metastasis (Hopkins, 2017).
Blockage of IL-8 (interleukin 8)
- luteolin
- apigenin
- vitamin D3
- quercetin
- curcumin (Jain, 2009)
CDK-6 inhibitor
More information about CDKs can be found in Peyressatre, 2015. It is an important target in brain cancers.
In clinical treatment a drug which inhibits CDK-6 is Palbociclib (Ibrance).
Blockage of Androgen Receptor (AR)
Androgens are a group of hormones that play a role in male traits and reproductive activity. Present in both males and females, the principle androgens are testosterone and androstenedione.
It is important target in prostate cancer, especially in early stages, where the cancer is hooked on androgen and is often treated with androgen deprivation therapy. In late stages though, the cancer becomes independent of androgen, but still remains a bit dependend on androgen receptors.
- curcumin

- urolithin (walnuts, pomegranate, rosemary)
You can cook yourself Fesenjan, which includes all of the above mentioned ingredients.
Wide spectrum anti-cancer effects
More information
Counihan, 2018. Cancer Metabolism: Current Understanding and Therapies
Agbarya, 2014. Natural products as potential cancer therapy enhancers: A preclinical update
Giunchi, 2018. The Metabolic Landscape of Prostate Cancer
Adenoid cystic carcinomas [ACC]. Main targets: PSPH, MCT4, SHMT1. Koo, 2015.
Demiray, 2016. c-Kit (tyrosine kinase receptor). Successful treatment of c-kit-positive metastatic Adenoid Cystic Carcinoma (ACC) with a combination of curcumin plus imatinib: A case report
Other useful information
Drug to drug interactions checker WebMD
Drug Interactions Flockhart Table. CYP enzymes. Link.
Sci-hub (link) – full lenght articles. If the link is not working, google “sci-hub” and you will find another mirror.
Cancer drugs A to Z list – CancerResearchUK
Drugs info Medscape
Lessening Chemotherapy Side Effects – Life Extension article.
Bevacizumab (Avastin) Drugs.com
Capecitabine (Xeloda). Drugs.com. Research graviola (Hansra, 2014) and ursolic acid (Prasad, 2012; Lombó, 2017).
Carboplatin DrugBank; Drugs.com; Medscape; cancerresearchuk
Cetuximab (Erbitux) MedScape; Drugs.com
Cisplatin DrugBank; Drugs.com; Medscape; cancerresearchuk
Cyclophosphamide DrugBank; Drugs.com; Medscape
Dacarbazine DrugBank; Drugs.com; cancerresearchuk
Docetaxel (Taxotere) DrugBank; Drugs.com; Medscape; cancerresearchuk
Doxorubicin (Adriamycin) DrugBank; Drugs.com; cancerresearchuk
Gemcitabine (Gemzar) DrugBank; Drugs.com; Medscape; cancerresearchuk
Oxaliplatin DrugBank; Drugs.com; Medscape; cancerresearchuk
Paclitaxel (Taxol) DrugBank; Drugs.com; Medscape; cancerresearchuk
Temozolomide (Temodal; Temodar) DrugBank; Drugs.com; cancerresearchuk
Topotecan (Hycamtin) DrugBank; Drugs.com
Glioblastoma – McConnell, 2019. Do Anti-Oxidants Vitamin D3, Melatonin, and Alpha-Lipoic Acid Have Synergistic Effects with Temozolomide on Cultured Glioblastoma Cells?
Interesting articles
- Lewandowska, 2014. Synergistic Interactions Between Anticancer
Chemotherapeutics and Phenolic Compounds and
Anticancer Synergy Between Polyphenols
Off-topic. Why we don’t have a cure yet?
They are two key elements of the protocol.
One is synergy. An effect arising between two or more substances that produces an effect greater than the sum of their individual effects.
Second is cancer-specific. Let’s call it “Buddies effect”. Some substances have effect only when you take them with some other substances. They need buddies for them to work. When you check studies on each substance of COC used alone, the results are not that promising. I would say there are even poor for some. But when you combine them, it may be a completely different story.
I believe this is also the main reason why we don’t have cure for cancers yet. The problem is that for a long time we have been trying to find one drug as a cure where there may never be a single substance as the cure.
First because cancer does not exist as a single disease. It is a large group of very different diseases.
Second, they are differences in patient’s bodies. Our genetic basis are different and thus our response to the treatments is different – important area studied by pharmacogenomics.
Third, even cancers with the same site of origin, like lung cancer, can be very different from one person to the other. Also pointing to differences in patients bodies.
Based on above, you can see how foolish are those internet testimonies starting with “I know a person who cured himself by….” and recommending you to do the same.
The structure of clinical trials may be blamed as it is usually focused on a single drug. Moreover the drug needs to work for most (here we have to consider how statistical significance works; they need to pass certain threshold which would mean success in the trial). And it needs to work for most without any other substances to help (they are being intentionally avoided as potential confounders).
But can there ever be a single drug which can cure cancers? I believe not.
Compare above to immunotherapy and something like CAR T-Cell therapy.
This is not seeking a drug which would cure. This is inventing a doctor who could be programmed to cure not cancers, but specifically the one cancer, the patient’s cancer.
Imagine such method to be applied universally, in a clinical trial, with only a single piece of programing (not tailored). It would fail.
CAR T-Cell is a major breakthrough, even though it has its limits. T-Cells can’t go everywhere, there are some “areas 51” where they are forbidden to enter. We have discussed the lactate shield and lacto-acidic wastelands around the tumors which are impenetrable for T-cells.
But what if the treatment is accompanied with the metabolic blockage?
Oxaliplatin, doxorubicin, paclitaxel and others cannot be programmed the same way as CAR T-cells can. There is fortunatelly the paradigm shift happening and CAR T-Cell therapy is one of those pioneers with great promise.
Only recently we have seen more attempts to test 2 or 3 drugs together at a single clinical trial (see point 4 and 5 in the article link). But metabolic blockage can employ tens of drugs with low toxocity, benefiting from their synergy and buddy effect.
Our basic design for finding cancer cure has set us to fail from the very begining, as cancers are too complex and patients are too different, for single drug to work.
Result is an extreme failure. We are at least attempting to figure out some regimens by trying to put some drugs together. But having only powerful toxic killers passing the faulty design as the “winners”, we can’t even mix them together because of unacceptable toxicities. At least we have come up with something like metronomic chemotherapy, to make best from the mess lasting over 60 years.
The flawed design of clinical testing led us not only to waste billions of dollars but we might have lost many extremely promising cancer drugs, which were not powerful enough when tested alone to provide any statistically significant benefits (the end points which have been set from the very beginning are favouring killer drugs, not “buddies”), but which could work wonders if only tried together with other drugs.
At workplace, we are obsessed with “team work”, but in cancer trials, we are forbidding it.
We have invented strong killers, which are unfortunatelly not strong enough to really do a complete kill – ending up in a vicious circle of a first line treatment – cancer developing resistance – second line treatment – cancer developing resistance – no more drugs available – palliative care – death.
Can metabolic blockage help to improve outcome of the standard oncological treatment? Can such attempt be even tested under current clinical testing setting? Imagine clinical study with over 30 different drugs and supplements.
Morgan, 2004 is a picture of 1990 – 2004 efforts, where billions of dollars were gone and results disappointing to say at least (compared to how much money was invested). Morgan study has some limitations, see critical review of Morgan in Segelov, 2006.
We were losing war on cancer up to until about 1990. Since 1990, we are starting to win for the very first time, though in a very slow pace.
See more in Gorski, 2020 “Contrary to what we are frequently told, we are not “losing the war on cancer” (2020 edition).
Q&A
Question 1
Is better to take metformin and berberine before meal (fasted) or after meal? (Kelly McDermott Davies on Facebook)
In the protocol metformin and berberine are taken at the same time (reason answered in Question 2), both after meal. The reason is that both drugs have stomach pain as possible side-effect when taking on empty stomach. I want to avoid any discomfort.
Is there any reason to use it before meal?
A valid reason would be significant increase in bioavailability, but as in Marathe, 2001: “Food does not appear to affect the bioavailability of either component to an appreciable extent.” (study on metformin).
Bioavailability of berberine is mainly influenced by usage of inhibitors of CYP3A4 and CYP2D6 and P-gp inhibitors (Long, 2016). But taking it with food also helps significantly (Persiani, 2014) “Food intake significantly increases berberine bioavailability”.
So based on above, I would recommend to use both after meal, to avoid often side effect and also to help berberine bioavailability.
Kelly points out to the article which says “That means it could be critical to administer mitochondrial inhibitors to cancer patients when their blood sugar is low, he says. That’s counter to how metformin and related medications are currently tested in cancer, because the protocol used to manage diabetes calls for the drugs to be taken immediately after meals.”
I would tend to disagree as the study wants to prepare patients for the kill phase. And it makes sense then to lower glucose first and then to use mitochondrial inhibitors. But this would be used as a short term solution before the kill phase. And it is absolutely valid idea.
My protocol is meant for a long run though and the glucose will be kept low after some time constantly – as we do starve phase. Not aiming for an immediate kill (and having no kill phase drug). Also berberine does probably accumulate through the time, so the effect will be more profound after a couple of months. But the idea is very interesting and maybe can be used for some specific chemotherapy / immunotherapy drugs – to help the drug to work better.
Question 2
Are people taking metformin and berberine together? I was told this was not a good idea as berberine interferes with metformin. (Jordan Tanko on Facebook)
I would think that taking both at the same time should have benefits over taken them separately in time. I believe those two are complementing each other, with some synergies.
Pang, 2015 mentions two studies where combination yielded better effects.
First study is Sheng, 2010:
“In a study conducted by Sheng and Xie, 60 cases were randomly divided into two groups and treated for three months: the treatment group received BBR (0.5 g, tid) in combination with glipizide (5 mg, bid) and metformin (0.5 g, tid), while the control group took glipizide (5 mg, bid) and metformin (0.5 g, tid) only; results showed that treatment group showed better efficacies in the levels of FBG, homeostasis model assessment of insulin resistance (HOMA-IR), TNF-α, IL-6, and CRP than those of control group (P < 0.05), indicating that BBR may be helpful to improve the disorders of glucose metabolism and insulin sensitivity.”
Second study is Yin, 2011:
“Yin et al. observed the effect of using BBR combined with metformin on primary T2DM. 60 patients were assigned randomly to treatment group and control group; BBR (0.3 g, tid) plus metformin (0.5 g, tid) were administrated orally in the treatment group, while the subjects in the control group took metformin (0.5 g, tid) alone for 24 weeks. Indicators of HbA1C, FBG, 2hPG, fasting insulin (FINS), and lipid series (CHO, TG, HDL-C, and LDL-C) were monitored. Results showed that the levels of HbAlC, FBG, 2hBG, FINS, TG, HDL-C, and LDL-C all decreased in both groups, and there was significant difference between before and after the treatment (P < 0.05). The treatment group showed better effects on the above indicators than those of the control group, and statistical difference was notable (P < 0.05).”
For anticancer effects. Zheng, 2017. “In addition, there is a potential synergy of BBR and MET. To our knowledge, this is for the first time to show that MET sensitized human lung cancer cell growth inhibition in response to BBR or vice versa.”

Question 3
Patrick, I see you are listing to take vid. D3 after dinner. COC recommends vit.D3 to be taken at breakfast and lunch time. Why do you think after dinner is best? (Jim Kirov on Facebook)
Vitamin D3 is added late to be close to melatonin due to their synergy. Synergy is a benefit for free and we should take it whenever an opportunity arises. See Cucina, 2010. Also Alkeraishan, 2019; Bizzarri, 2003; Almalky, 2019.
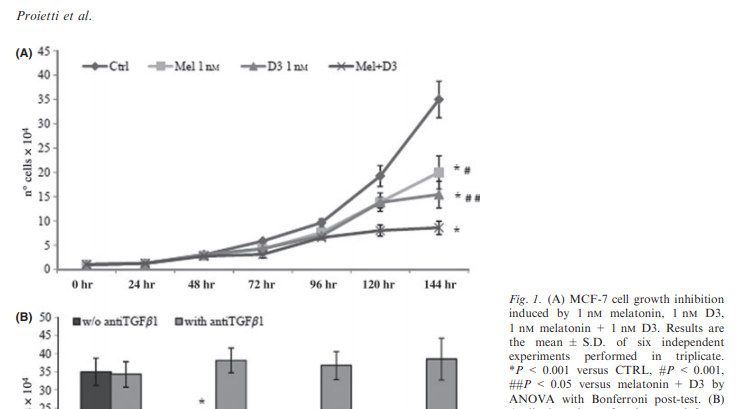
And it also may improve sleep by improving effects of melatonin (Placzek, 2019).
Question 4
Hi Patrik, I recently read several articles that do not recommend taking milk thistle alongside other meds and supplements as it might decrease their effect. In those articles, metformin and atorvastatin were cited several times. Would you have any thoughts on this topic? Thx in advance, Ray
Part of the answer is explained here in the article. As atorvastation is metabolised (out of body) by CYP3A4, it means when you block CYP3A4, more of atorvastatin is getting into blood stream = the dose will be more potent (which might increase its side effects risks). But this is to a more extent with Lovastatin and Simvastatin, not so much with Atorvastatin.
For your worry about potential decrease in the effect, you would need to take inducers of CYP3A4 like St John’s Wort. Milk Thistle is an inhibitor, so it won’t decrease the effects. I have been afraid the effects might be too strong in my protocol so I suggested to limit dose to 20mg when co-administered with other supplements. It might not be necessary, but I want to be on a safe side. We would still have good efficacy with 20mg dose, but less risk of side effects. Summary at Medsafe article.
Atorvastatin bio availability is also influenced to some extent by P-glycoprotein and OATP C. Milk Thistle is not a potent inhibitor of P-gp (Gurley, 2006; Kawaguchi-Suzuki, 2014).
For metformin, it does not have any interactions with Milk Thistle. Metformin is not metabolised by CYP enzymes. The only thing they have common is that Milk Thistle may also lower blood glucose. So diabetes patients need to be careful to avoid lowering glucose too much.
Written by: Patrik Schoupal
The latest update: 17th of October, 2020
First published: 10th of February, 2020
All content on the page is free.
Though if you like to buy me a coffee
PayPal.Me/fullmetabolic
© 2020 Patrik Schoupal All Rights Reserved
Disclaimer
While I strive to make the information on this website as timely and accurate as possible, I can not make claims, promises, or guarantees about the accuracy, completeness, or adequacy of the contents of this site, and I expressly disclaim liability for errors and omissions in the content of this site. I am not a doctor. I do not diagnose, prescribe, treat, or cure. I try to provide/collect information (for educational purposes) based on my research and the research of others. I do not suggest anyone follow my advice without getting the advice of a qualified health professional.
Some information in this article are experimental hypothesis. Meaning they are opinions based on limited evidence, not generally acknowledged facts.